

What does an organization do when it achieves it’s goal? You might think it would disband in triumph, but that’s not the case with The March of Dimes.
The organization was created by President Franklin Roosevelt to combat the scourge of polio and was spectacularly successful in its goal. Polio has been nearly wiped off the face of the earth because of the polio vaccine. Instead of disbanding, however, the organization has sought to perpetuate itself by finding another cause.
For a while, The March of Dimes concentrated on “birth defects”: congenital medical anomalies and illnesses. They have not been nearly as successful in addressing that problem because it is complex and multi-factorial. Now they’ve moved on to prematurity. It is also a complex multi-factorial problem that does not lend itself to easy answers. The March of Dimes has scored no successes in preventing prematurity, but they’re undaunted. Unfortunately, instead of greater efforts to address the major problem of extreme prematurity that is responsible for a large proportion of neonatal deaths, The March of Dimes has chosen to misrepresent the problem in order to be seen as doing something. The misrepresentations are disingenuous and, in some cases, border on outright dishonesty.
The March of Dimes has chosen to misrepresent prematurity as being caused by early elective delivery. While early elective delivery poses risks, it also has significant benefits (reducing the stillbirth rate) and, in any case, is only a tiny contributor to the problem of prematurity. I suppose one could argue that hyping the issue of early elective delivery is like looking for your keys under the streetlamp even though you dropped them elsewhere. The answer is not likely to be there, but at least that’s where the light is.
I can think of no good reason the be dishonest about prematurity and race, however, and The March of Dimes is thoroughly dishonest on that point. Black African ancestry is a major risk factor for prematurity, but the MOD has not simply ignored this reality, they started denying it, too.
The MOD has been publishing a yearly “report card” on prematurity. The report card is rather farcical since while claiming to grade states on prematurity rates, it is basically grading them by the proportion of African-Americans in each state.
According to NBC.com:
Vermont led the nation with just 8.7 percent of births coming before 37 weeks gestation. Alaska, California, Maine, New Hampshire and Oregon had rates of 9.6 percent or lower, the target recommended by the March of Dimes…
The states with the highest rates of preterm birth are Mississippi (17.1 percent), Louisiana (15.3 percent) and Alabama (14.6 percent). If they were countries, they would be among the 14 worst of the 184 for which data are available, according to the U.N. report. The global average is 11.1 percent…
The high U.S. rate for preterm births is often blamed on the nation’s racial, ethnic and economic diversity, said McCabe [medical director of the March of Dimes], “but the California example refutes that.”
California, with half a million births each year, “has an incredibly diverse population, but it set up policies and procedures to make reducing preterm births a priority,” he said.
Not exactly.
The scatter plot below compares prematurity rates to the proportion of African-American’s within each state.
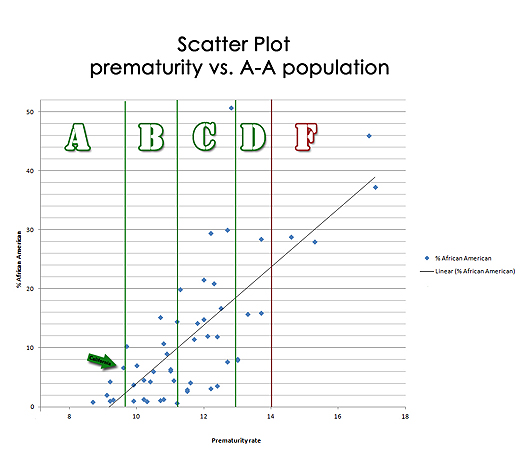
As you can see, there is a strong correlation between prematurity rates and the proportion of African American in each state. I calculated a correlation coefficient (Pearson’s r) of 0.75. The whitest states have the lowest prematurity rates and the blackest states have the highest prematurity rates. In other words, the whitest states merit an A grade, while the blackest states are awarded F’s.
The arrow identifies the data point for California. Contrary to Dr. McCabe’s claim that California refutes the relationship between race and prematurity, California actually has a very low proportion of African Americans, corresponding to its low prematurity rate.
Why is any of this important?
We aren’t going to be able to solve the problem of prematurity if we aren’t honest about the reality of prematurity. Yes, there is an iatrogenic component to American prematurity rates, but this is a trivial aspect of the problem. Not to mention that reducing iatrogenic prematurity has risks of its own.
More importantly, the strong correlation between race and prematurity suggest a major genetic component. We should be aggressively searching for a genetic basis for prematurity instead of pretending that it doesn’t exist. But that, of course, it hard, and The March of Dimes would prefer the easy way out, grandstanding by “grading” states on prematurity rather than do the difficult work of solving the actual problem.
Addendum:
March of Dimes state by state prematurity statistics can be found here: http://www.multivu.com/players/English/59684-march-of-dimes-75th-anniversary/
African-American state by state population statistics can be found on Wikipedia: http://en.wikipedia.org/wiki/List_of_U.S._states_by_African-American_population
