In the wake of the Karen Carr homebirth debacle, homebirth advocates have trotted out a classic homebirth lie: “Babies die in the hospital, too.”
It’s time to set the record straight. No, homebirth advocates, otherwise healthy babies DON’T simply drop into the obstetricians hands unexpectedly dead. Otherwise healthy babies DON’T unexpectedly drop dead for lack of appropriate medical equipment and emergency personnel. The babies whose mothers would be eligible for homebirth (full term, no medical complications of pregnancy, no pre-existing medical conditions) hardly ever die during or after a hospital birth.
The following chart, adapted from Infant, neonatal, and postneonatal deaths, percent of total deaths, and mortality rates for the 15 leading causes of infant death by race and sex: United States, 2007 makes that clear. The chart shows neonatal death rates by cause.
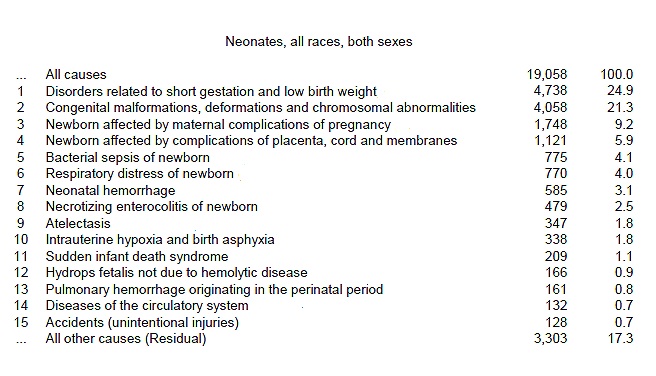
As you can see from the chart, more than 50% of all neonatal deaths are due to prematurity and its complications (respiratory distress, necrotizing enterocolitis) and congenital anomalies. These babies, of course, are not otherwise healthy full term babies.
Consider the other major causes:
Maternal complications of pregnancy- not homebirth candidates
Complications of placenta and membranes (i.e. placenta previa, abruption, chorioamnionitis) – not homebirth candidates.
Together, these causes account for 68% of all neonatal deaths.
The fact is that neonatal death in otherwise low risk women in the hospital setting is quite rare. The best estimate that we can make based on CDC data is a neonatal death rate of 0.4/1000 in low risk, white women at term. That figure actually includes congenital anomalies, which account for nearly 50% of term deaths. In other words, the death rate for otherwise healthy babies is in the range of 0.2/1000 or 2 deaths for every 10,000 births.
Considering that there are approximately 10,000 CPM attended homebirths per year in the US, we would expect only two homebirth deaths per year. Yet in 2009 there were 4 neonatal deaths in the state of Colorado alone in 2009!
Otherwise healthy babies do not die in the hospital, too. Yes, “some” babies die, but those are born prematurely or born to women who would never have been candidates for homebirth.
Existing scientific studies and state and national data estimate that homebirth triples the rate of neonatal death, but that considerably under-counts homebirth deaths, which often appear in the hospital statistics, not the homebirth statistics. The real risk of homebirth is larger, possibly much larger.
Is it any wonder that MANA (the Midwives Alliance of North America) is hiding their homebirth death rates? Those death rates, which also under-count homebirth deaths, must be appalling indeed.