American homebirth advocates continue to celebrate the recent publication of homebirth studies from Canada and the Netherlands. Evidently, they have failed to grasp the central lesson of both studies: homebirth can only be safe when practiced by highly educated, highly trained midwives under rigorously controlled conditions. Since this is in direct opposition to the philosophy of American homebirth, it is not clear what advocates are celebrating.
Reading the Canadian and Dutch studies makes it clear that Canadian and Dutch midwives don’t “trust birth.” There is none of the prattle traditionally associated with American homebirth. No babbling about how birth “is not a disease”; that women’s bodies are “designed” for birth; that babies are “not library books,” due on a certain day.
In fact, the fundamental premise is exactly opposite: birth is inherently dangerous and great care must be taken to prevent, diagnose and manage complications. Practitioners must adhere to the tenets of modern obstetrics. Consistent with that premise, both countries mandate rigorous education and training of midwives. Midwifery is a university degree; midwives are trained for both hospital and home; and significant education and training is devoted to handling complications. No one pretends that homebirth midwives are “experts in normal birth,” as if such a thing were even possible. There is no such thing as a homebirth midwife. All midwives attend births in the hospital and at home.
In contrast, American homebirth midwives are grossly undereducated and undertrained. The CPM designation (certified professional midwife) is a post high school certificate program, not a college degree. Most courses are not eligible for transfer college credit because they are foolish: homeopathy, flower essences, gem energy, etc. There is no training in managing complications because there is no hospital training. Clinical training is nothing more than an apprenticeship to an older midwife.
Keeping with the premise that childbirth is inherently dangerous, both Canada and the Netherlands have strict criteria for homebirth eligibility. Virtually anything that raises the risk of potential complications results in disqualification for homebirth: no breech, no twins, no postdates, no pre-existing conditions or conditions arising during pregnancy. These are not considered variations of normal; they are recognized as abnormal and treated accordingly.
American homebirth midwives, in contrast, like to pretend that virtually anything that happens naturally is normal. Postdates pregnancy? That happens naturally, so the baby must “know” when to be born. Labor stalled at 7 cm for 5 hours? No problem, just keep waiting for labor to naturally pick up. American homebirth midwives routinely ignore due date, blood pressure, glucose tolerance, colonization with group B strep, virtually that occurs naturally during pregnancy.
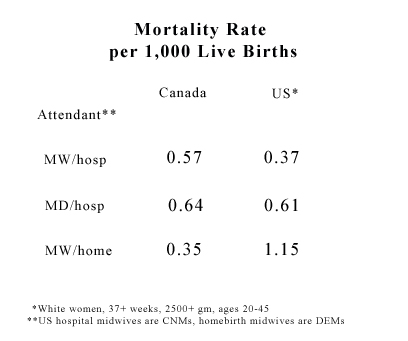
The dismal mortality statistics of American homebirth midwives reflect their poor understanding of childbirth. Homebirth with American homebirth midwives has approximately triple the neonatal mortality rate of homebirth in Canada or the Netherlands. Homebirth with American homebirth midwives has almost triple the neonatal mortality rate for low risk hospital birth in the US.
Both the Canadian and Dutch studies have methodological problems that raise questions about their conclusions. The Canadian study has an unusual way of calculating perinatal mortality, and the Dutch study points out that homebirth is as safe as hospital birth in the Netherlands without addressing the fact that the homebirth population is much lower risk than the hospital population. Nonetheless, the neonatal death rates for homebirth in both studies is dramatically lower than for homebirth with an American homebirth midwife.
Homebirth with an American homebirth midwife can never be safe unless the midwives are held to a higher standard. Their level of education and training must be brought up to the same level as midwives in every other first world country. Homebirth must be subjected to the same eligibility requirements as in other first world countries. Unless standards are raised, babies will continue to die unnecessarily at births attended by American homebirth midwives.