The folks at Lamaze are at it again. Amy Romano of the Lamaze blog Science and Sensibility has utterly misrepresented a new study. Indeed, the author of the study left a comment on her blog explaining exactly how she misrepresented it. But Amy Romano is not cowed by anything as unimportant as the truth. She’s not going to change her post. Presumably that’s because the original objective had nothing to do with science and everything to do with demonizing epidurals.
The paper in question appeared online at the British Journal of Obstetrics and Gynaecology website. Intrapartum risk factors for levator trauma by Shek and Dietz looks at the effects of childbirth on the levator ani, muscles that support the pelvic contents.
The authors were attempting to determine why vaginal delivery increases the risk of pelvic organ prolapse and related symptoms in older women. Some women sustain visible damage to the levator ani muscles (macrotrauma) resulting in a gap between the muscles that the pelvic organs can fall through. However, many women who have no evidence of mactrotrauma go on to develop pelvic organ prolapse. The mechanism seems to be damage to the substance of the muscle itself (microtrauma) that leads to weakening and stretching of the muscles. That can also lead to widening the gap between the muscles, a weakening that may only be noticeable when the intraabdominal pressure is increased, such as when the woman coughs or sneezes.
Sounds reasonable, right? But not to the folks at Lamaze. Amy Romano makes a series of empirical claims, all of which are demonstrably false.
We put “microtrauma” in quotes because no one has ever defined or determined the prevalence of this “condition”. The researchers invented it themselves!
Levator microtrauma is an example of a surrogate outcome (sometimes referred to as a surrogate endpoint)… [S]ome surrogate outcomes are extremely poor predictors of actual outcomes, and changing clinical practice based on studies that report only surrogate outcomes can be a major threat to patient safety if the therapy introduces other risks…
… [T]here is absolutely no data whatsoever linking the author’s definition of microtrauma to pelvic organ prolapse or other important pelvic floor problems such as incontinence or sexual dysfunction.
Wrong, wrong and wrong. If such claims sound familiar it’s probably because they employ the same language I have used to describe the blather than emanates from natural childbirth advocates: they make up “facts” to suit themselves. Did Romano want to turn the tables? If so, it was a spectacular failure as she simply demonstrated once again that NCB advocates make up “facts” to suit themselves.
What’s the truth? Muscle microtrauma can occur in any muscle, is widely mentioned in the scientific literature and has been mentioned in connection with the levator ani muscles in previous scientific papers. No one knows exactly how the levator ani muscles weaken in the aftermath of childbirth, but microtrauma is a very plausible explanation.
Levator ani microtrauma is not a surrogate outcome since the study was designed specifically to look at all possible ways that the levator may be damaged by vaginal delivery.
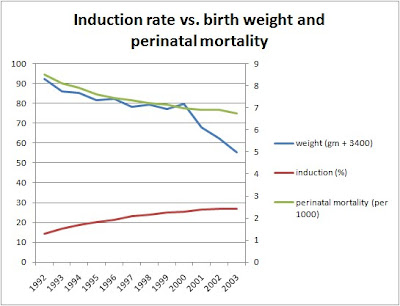
Why so much fuss over a study about muscle damage and prolapse? Why the tremendous effort to misrepresent the study by making up false claims? The answer is buried at the end of the study. When looking at a variety of factors that increase or decrease the risk of levator trauma, authors mentioned in passing that epidurals appear to be protective.
Oh, no! Epidurals are bad, bad, bad. Lamaze can’t let anyone get away with reporting any benefits from epidurals so the authors and their research must be discredited at all costs, truth be damned. And some made up medicine must be thrown in:
… Maybe doing away with coached pushing, fundal pressure, episiotomy, and supine positioning might be the better strategy. Maybe postpartum exercises can help reverse changes associated with pregnancy and vaginal birth so they don’t turn into symptomatic pelvic floor problems.
No evidence? No problem.
Dr. Dietz responded:
I’m the senior author of the study discussed by you. After 25 years of research in this field it still depresses me how excited people get when it comes to research that may affect the choices made by women in childbirth. There is way too much ideology and zealotry out there for a rational discussion. Amy Romano, you seem to intuitively know what’s right- saying: “Maybe doing away with coached pushing, fundal pressure, episiotomy, and supine positioning might be the better strategy.” How do you know? Where is the data?
And how do you know what ‘pelvic floor damage’ is? By all means do check my website if you really want to know:
http://web.mac.com/hpdietz1/iWeb/Site/Welcome.html
It seems you’re interested in those issues, and good on you for that. I’d be happy to answer any questions you may have, and I promise not to be prejudiced in any way. We all want the same: healthy mums and healthy babies. Just try and avoid the zealotry please.
Dr. Jeff Livingston wrote to encourage Romano to correct her mistakes:
… I am hoping you make a statement correcting your representation of the study so that we don’t spread false information since all of us are simply promoting science and patient safety through patient education. You have a large audience and I would not want them to get the wrong idea. I like this paper because it was simply thought provoking. I do a lot of pelvic reconstruction surgery. More papers like this looking at the basic science underlying pelvic floor damage will help us improve our understanding and surgical techniques in the future. That is how I will apply the paper in practice. It didn’t really speak to me about labor management.
So will the fact that the author and others eviscerated Ms. Romano’s “analysis” cause her to correct her misrepresentations and falsehoods? No way!
I’m not sure what you think I misrepresented…. But as of now I stand by everything I wrote.
I have written before that a key characteristic of science, as opposed to pseudoscience, is that all possible outcomes are allowed. That’s why “intelligent design” is not science; there is no evidence that would lead it’s advocates to announce that there is no “intelligent designer.” The conclusion is predetermined.
Romano’s analysis of this scientific paper veers perilously close to pseudoscience. It starts with an unalterable conclusion – under no circumstances can epidurals be beneficial. It then precedes to trash the study, making demonstrably false claims about microtrauma, for the SOLE purpose of insuring that no one credits the observation that epidurals may be protective. Finally, with absolutely no data, it asserts that the current recommendations of NCB advocates would surely be protective.
I think Romano owes the authors of the study an apology and a correction. She deliberately mischaracterized their work to fulfill a private agenda of demonizing epidurals.