![]()
Imagine the following scenario:
The drug company Profits-R-Us introduced a new medication to treat the common cold, Sneeze-Ease. Shortly after its introduction, doctors beginning noticing a number of unexpected deaths of people who were previously well. The only thing that connected these deaths was the fact that all the people who died unexpected had ingested Sneeze-Ease within 48 hours of their deaths. The FDA demanded that Profits-R-Us reanalyze their data to determine if the new medication was responsible.
The marketing department of Profits-R-Us sent out the following press release:
Profits-R-US (PRU) collects post marketing information on all its medications. In 2006, shortly after the introduction of Sneeze-Ease PRU received reports of 5 deaths associated with Sneeze-Ease; in 2007 it received reports of 5 deaths; in 2008 it received reports of 7; and in 2009 it received reports of 9.
PRU collected brief stories about the situations surrounding the demises. Based on the information provided, these data suggest that Sneeze-Ease can be ruled out as a causative factor in the death in all but one of these deaths, although even with this one it is not clear whether the hospital would have been able to save the patient if he had gotten there in time.
The mission of Profits-R-US is to provide safe and effective medication. PRU declares and affirms that Sneeze-Ease continues to be a safe and viable choice for treating colds.
Now imagine that you learn that PRU has been withholding some additional information. In 2010, 15 patients died after ingesting Sneeze-Ease, and in 2010 14 more people died.
So at the exact same time that PRU is publicly affirming the safety Sneeze-Ease it is in possession of new information that is even more damning than the original information.
Were a drug company found to be behaving like that, we would be disgusted by the duplicity and unethical behavior of it’s executives.
We should be equally disgusted by the duplicity and unethical behavior of the Colorado Midwives Association (CMA) because it is just performed the exact same stunt, trying to explain away their appalling death rates.

Stung by my persistent criticism of the extraordinary death rates for planned homebirths attended by Colorado licensed midwives, the organization is attempting to protect its “product,” at the expense of the safety of babies and mothers.
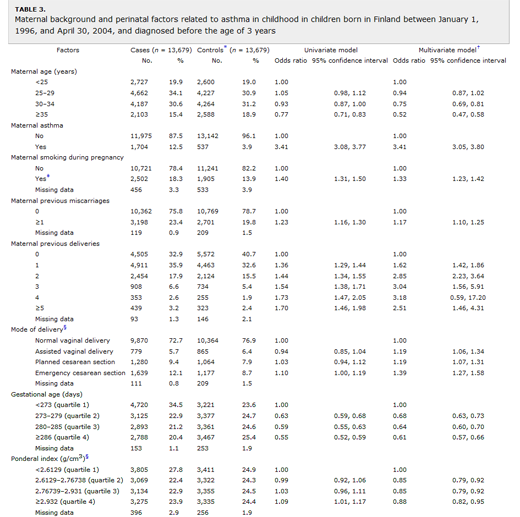
The above chart shows the death rates for planned homebirths attended by licensed Colorado homebirth midwives from 2006-2011.
In violation of Colorado state law, the homebirth midwives did not release their 2010 and 2011 statistics. They were obtained by filing a Colorado Open Records Request, forcing the midwives to release them. I wrote about the 2010 data a few weeks ago. This post marks the first public disclosure of the 2011 data.
On their website, under the title Homebirth Safety in Colorado, issued almost exactly the same statement as above.
The Colorado Department of Regulatory Agencies (DORA) Office of Direct-Entry Midwifery Registration collects this information via a survey administered each year to midwives seeking renewal… In 2006, the survey reported 5 perinatal deaths; in 2007 it reported 5; in 2008 it reported 7; and in 2009 it reported 9. Over the last 6 years, Colorado has averaged between 40 and 60 Direct-Entry Midwives attending between 500 and 700 homebirths per year.
Based on the information provided, these data suggest that planning a home birth can be ruled out as a causative factor in the death in all but one stillbirth during labor, although even with this one it is not clear whether intervention such as a Cesarean section would have saved the baby …
The mission of the Colorado Midwives Association is to support and promote the option of homebirth for childbearing families in the state of Colorado. The Colorado Midwives Association declares and affirms that homebirth continues to be a safe and viable choice for women with healthy, low-risk pregnancies when attended by a Colorado Registered Midwife.
It is deceptive:
* By failing to provide a comparison rate for comparable risk women giving birth in the hospital, the Colorado Midwives Association makes it impossible to determine whether the death rates are acceptable. The CMA does not disclose that the overall perinatal mortality rate for the entire state of Colorado (all races, all gestational ages, all pregnancy complications, all pre-existing medical conditions) of 6.3/1000. So the homebirth death rate is extraordinarily high.
It is unethical:
*The CMA fails to disclose the information for 2010 and 2011, showing that the appalling death rate has risen even higher than they acknowledge.
It is disgusting:
* It is indicative of the mendaciousness of homebirth midwives who are more concerned with promoting their “product” than whether babies live or die.
Colorado homebirth midwives are no different from the theoretical executives of Profits-R-Us. They will say whatever it takes, hide whatever it takes and tell whatever falsehoods it takes to continue making money despite the fact that patients are dying.