Bullies always go for what they perceive as the weakest link.
UK Midwives are very upset with me, upset with what I’ve written and even more upset because it’s all true.
Recently I’ve written:
Byrom ought to be ashamed of herself for the derisive way that she dismissed the father of a baby who died as a result of midwifery incompetence. But that would involve kindness, compassion and respect, something in woefully short supply among UK midwives.
Imagine my surprise, then, to find that Byrom has edited a book about kindness, compassion and respect in maternity care.
Apparently, what she means is kindness, compassion and respect for those who agree with her and vicious, disrespectful neglect of anyone else who dares criticize Byrom and her colleagues.
2. Being a UK midwife means you never have to say you’re sorry:
In the wake of the Morecambe Bay Report, which investigated the deaths of 11 babies and a mother and placed blame squarely on a midwifery culture that valued “normal birth” above all else, you might think that UK midwives would be in a mood of somber reflection about their deadly philosophy.
You would be wrong.
Yesterday I entered the weekly Twitter chat at the hashtag #WeMidwives hosted by the Royal College of Midwives (RCM). If I hadn’t been there myself, I would not have believed the smugness, meanness, utter lack of reflection and inability to tolerate criticism that characterized the Royal College of Midwives and it’s members.
Apparently, no matter how many dead babies, no matter how many dead mothers, being a UK midwife means you never have to say you’re sorry.
3. Midwives are wrong to fight fear in childbirth; it’s a lifesaving gift.
UK midwives’ desire to “fight fear” in childbirth is both grossly hypocritical and stunningly immoral. They want women to fear everything they can’t provide and they want women to ignore the legitimate, protective fear that they or their babies will be injured or die in life threatening emergencies that are all too common in childbirth.
4. And I’ve been participating quite vigorously in the comment section on The Guardian piece I loved being a midwife but bullying, stress and fear made me resign:
… I have never seen midwives or their defenders address is that “normal birth” is a construct of midwives, created for the benefit of midwives without any input from the majority of women. It is wrong for a provider to privilege process over outcome. A safe outcome should be the sine qua non of maternity care. A particular way of giving birth should NEVER be the goal except when a specific individual woman chooses it as HER goal.
Her body, her baby, her birth, NOT —- as it is now — her body, her baby, and the unmedicated vaginal birth that the midwife prefers, which never requires calling in anyone who might not support the midwife.
UK Midwives are very unhappy but apparently incapable of rebutting my claims or addressing my arguments.
Instead, they appear to be pressuring James Titcombe, whose baby died at the hands of midwives in Morecambe Bay, by sending the Twitter conversation about their unhappiness with his associations directly to his employer.
It appears that he tweeted a link to something I wrote. It’s hard to tell because he deleted it in response to their reaction.
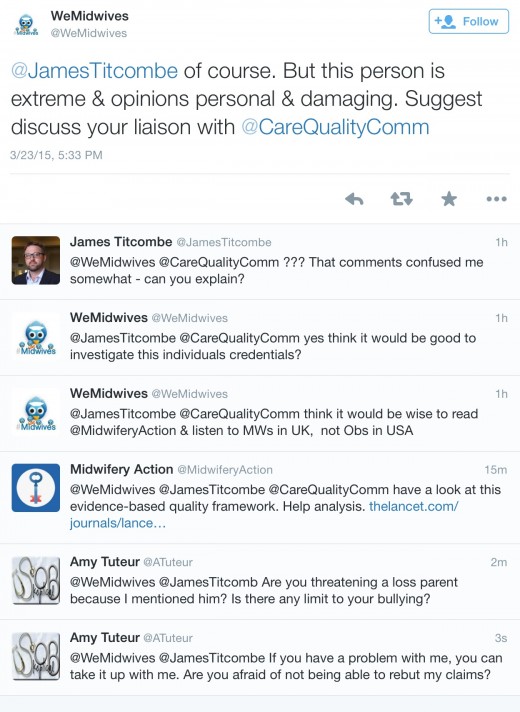
WeMidwives
@JamesTitcombe of course. But this person is extreme & opinions personal & damaging. Suggest discuss your liaison with @CareQualityComm
And:
WeMidwives @WeMidwives 2h2 hours ago
@JamesTitcombe @CareQualityComm think it would be wise to read @MidwiferyAction & listen to MWs in UK, not Obs in USA
So WeMidwives thinks it is perfectly acceptable to threaten a loss parent. That’s bad enough.
Why are they threatening him anyway? Because they think he can pressure me to stop.
They don’t know me very well, do they?
Let me state unequivocally (since they did “report” him by sending the tweet to his employer) that James Titcombe has nothing to do with what I’ve written in the past week about UK midwives. I don’t consult him; he doesn’t consult me; he has no control over what I write.
And let me publicly apologize to him for being a target of the wrath that UK midwives have for me. If they have a problem with me, they can address me directly.
Elsewhere in the Twitter feed, they claim:
we aren’t prepared to associate with this person-has no respect or credibility in UK
If that were the case, they wouldn’t be worried about me, and they are worried enough to threaten an innocent bystander.
Maybe someone familiar with the UK medical system can help me out here.
How can these midwives be so brazen as to pressure a loss parent publicly on social media?
Is their union so powerful that it doesn’t matter how they treat people?
Is anyone powerful enough to hold UK midwives to account for the deaths at their hands and for their outrageous, bullying behavior?
Or will the babies and mothers who die at the hands of UK midwives be buried twice, once in coffins in the ground and again by obliterating their deaths from public consciousness?