Let’s do a little thought experiment.
Imagine for a moment that Big Pharma has invented a new pain reliever, Fly-ox. Fly-ox is terrific. It provides excellent pain relief to many who didn’t like standard pain medications, and patients are singing its praises. Fly-ox is such a big seller that it becomes a major source of income for Big Pharma. The stock price of Big Pharma soars and the stock holders are thrilled.
At first, Fly-ox is not in the formulary of insurance covered drugs, so patients have to pay out of pocket. But Big Pharma has been working assiduously to gain approval from each individual insurance company so the insurance company will pay the full price for Fly-ox, instead of the patient. They’ve had some successes.
There’s just one teensy, weensy problem:
In studies that done by Big Pharma, but carefully removed from its FDA application, Fly-ox increased the risk of death.
At first the executives at Big Pharma thought it might be a mistake and that’s how they justified to each other leaving that information out of the application that led to FDA approval for Fly-ox. But in the past 5 years, Big Pharma has funded secret studies that have shown over and over again that Fly-ox leads to increased deaths, far outstripping deaths caused by side effects from other pain relievers.
The executives at Big Pharma stay mum about the increased risk of death, hoping that no one will notice, but eventually doctors do notice and reporting the deaths to the FDA. The FDA issues a black box warning about Fly-ox, and the survivors of those who died after taking Fly-ox start filing law suits. During the discovery phase of the lawsuits, plaintiffs lawyers subpoena the internal emails of Big Pharma and find prolonged email exchanges about how to keep the news of Fly-ox deaths from the public and the public relations campaign mounted to convince patients and doctors to ignore the FDA warning and continue using Fly-ox. Not surprisingly, juries start awarding big payouts when they learn that Big Pharma knew all along that Fly-ox led to preventable deaths, deaths that Big Pharma worked assiduously to conceal.
That’s reprehensible, right?
Now let’s change the story just a little. Replace “Big Pharma” with MANA (the Midwives Alliance of North America), the organization that represents homebirth midwives, and replace “Fly-ox” with homebirth:
MANA offers a new option, homebirth. Homebirth is terrific. Homebirth provides warm, supportive care to many who didn’t like standard hospital childbirth, and mothers are singing its praises. Homebirth is so popular that it becomes a major source of income for MANA. The public profile of MANA soars and homebirth midwives and advocates are thrilled.
At first, homebirth is not covered by insurance, so patients have to pay out of pocket. But MANA (and its sister organizations like The Big Push) has been working assiduously to gain approval from each individual insurance company so they will pay the full price for homebirth, instead of the patient paying. They’ve had some successes.
There’s just one teensy, weensy problem:
In studies that done by MANA, but carefully concealed from American women, homebirth increased the risk of perinatal and neonatal death.
At first the executives at MANA thought it might be a mistake and that’s how they justified to each other leaving that information out of their public pronouncements about the safety of homebirth.. But in the past 5 years, has continued to collect data that have shown over and over again that homebirth leads to increased deaths, far outstripping deaths that occurred in hospital childbirth
The executives at MANA stay mum about the increased risk of death, hoping that no one will notice, but eventually doctors do notice and begin reporting the deaths. The executives at MANA begin a public relations campaign to convince mothers to ignore the increased death rate and continue to choose homebirth.
In other words, MANA and its executives, are behaving just like Big Pharma, hiding evidence of death caused by its product in order to keep making money from it.
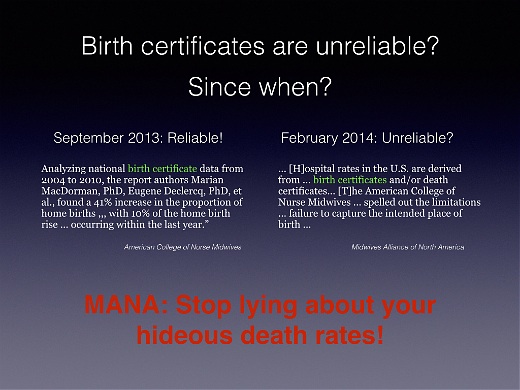
The MANA public relations campaign is a wonder to behold. In fact, MANA is even more brazen than Big Pharma. Big Pharma omitted mention of deaths from its papers about Fly-ox, while MANA actually reveals the 450% higher death rate from homebirth and then brazenly asserts that the death rate is evidence of “safety.”
MANA has its executives and friends stringing together mistruths, half truths and outright lies in an effort to blind their followers to the simple truth that homebirth kills babies.
Melissa Cheyney, Wendy Gordon, and Judith Lothian, I’m looking at you, among others.
Frankly, ladies, I don’t know how you can stand to look at yourself in the mirror. Your behavior is so unethical that it takes my breath away:
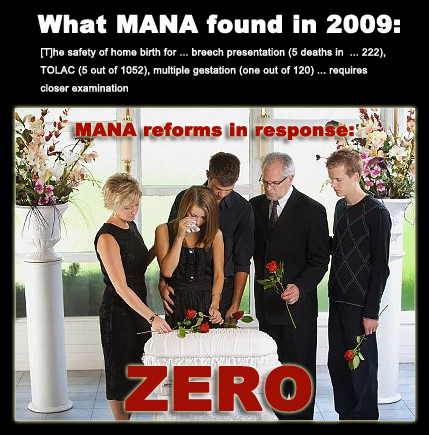
You have known FOR YEARS that homebirth increases the risk of perinatal and neonatal death, but you have hidden that information from American women.
You refused to release your hideous death rates because you were fully aware that they demonstrate beyond a shadow of a doubt that homebirth kills babies who didn’t have to die.
You are lying through your teeth about the meaning of the statistics revealed in your latest paper.
You are behaving exactly like big Pharma, throwing women and babies under the bus in an effort to preserve your income and your prestige within the homebirth community.
Your efforts to hide the dangers of homebirth are grotesque, and if you had an ounce of integrity, you’d be ashamed of yourselves.
But then, if you had an ounce of integrity, you wouldn’t be behaving like Big Pharma in the first place, would you?