As the year 2011 draws to an end, I’d like to review the year in homebirth. In this post, I review the homebirth deaths that I wrote about in the past year. In future posts, I’ll address the state and national statistics released this year as well as the homebirth studies that were published in 2011.
First, the homebirth deaths:
1. Attempted VBA3C
Initially reported on a message board:
A girl who I went to college with had a baby around 10 last night & both are in critical condition. This is her 4th baby. She had 3 previous c-sections & was trying for a VBAC homebirth. Her uterus ruptured in several places & she lost a lot of blood. She is intubated & had 2 blood transfusions. She isn’t out of the woods yet, by any means. The baby was born blue & unresponsive, was resusitated, but showing signs of possible brain damage. She was flown to a different hospital than her mom. The baby is being kept in some sort of induced unconscious state currently. Please keep Lori & baby Vera in your thoughts & prayers!! Thanks.
From the blog of a family member:
Update (2/3/11): According to the neonatalogists “…the MRI showed that a large amount of fluid had collected (hydrocephalus) and was putting pressure on parts of the brain, actually moving sections into different areas (herniation). The EEG showed minimal electrical activity from the cerebral hemispheres. The neurologist stated that there is some brain swelling as well as significant brain damage in a large part of her brain, but she is NOT brain dead. Vera still has some reflexes. What they believe Vera has is HIE, Hypoxic Ischemic Encephalopathy.”
Update (2/12/11): Vera died last night.
2.Arrest of midwife Amy Medwin
You might think that this would be an opportunity for soul searching in the North Carolina homebirth community, but you’d be wrong. The North Carolina Friends of Midwives and the Charlotte chapter of the International Cesarean Awareness Network (ICAN) view this as an oppportunity to promote the interests of CPMs.
The latest news reports indicate that Medwin’s current arrest was prompted by TWO bad outcomes in one month. The first case was an intrapartum death in which Medwin attended the labor but claims she left before the birth of the dead baby. The second is the case discussed above in which the baby is still hospitalized and fighting for its life.
3. Joseph
Alicia’s son Joseph died in the aftermath of a homebirth. Writing on Mothering.com, Alicia explains:
One month ago I gave birth at home to a beautiful 9lb 9oz baby boy named Joseph Phoenix, but he decided that he did not need to stay long in this world and he died the next day…
He decided? Not exactly.
According to a memorial on Flicker:
[The baby] was born at 10:05 AM on February 13, 2011. He was not breathing when he was born because his arm had pinched off his umbilical cord as he descended. The hospital re-started his heart but he was already gone, as later tests showed no brain activity…
He did not “decide” to die. He died because of profound hypoxia during labor that went unnoticed and untreated.
4. Midwife Karen Carr
Carr’s guilty plea to felony charges came in the wake of presiding over the death of a breech baby who’s head became stuck for more than 10 minutes before Carr even bothered to call 911.
The baby’s position wasn’t the problem, Carr said; the problem was that the baby’s head became stuck.
That is the obstetric equivalent of insisting that ‘it wasn’t the fact that I pushed him off a ten story building that killed him; the problem was that he hit the ground.”
5. Complaining that doctors play the “dead baby card“
After that experience and the regret of not trusting my instinct, I told DH that we’d be having no more babies unless I was able to plan a homebirth for the next one. I’m full-term with baby #3 and hoping to have an awesome HBA2C story in the next month! No matter how the birth turns out, I appreciate having a care provider who understands that each pregnant mother is an individual who is capable of researching and making her own decisions about “HER” body and child…
The mother began labor spontaneously at 41 1/2 weeks, labored for 24 hours and apparently delivered vaginally the day before yesterday.. The baby was born not breathing. Subsequent evaluation revealed meconium aspiration and catastrophic brain damage due to lack of oxygen. The decision was made to take the baby off life support.
The baby is dead.
6. Birth center death
The mother claims:
I don’t ever want anyone to fear a VBAC, or to fear going over their due date, or to fear having their baby in a birthing center because of our situation. Those things had nothing to do with what happened to our little angel, and there isn’t anything that could have been done to prevent it either.
Not exactly. Had the mother had an elective repeat C-section at term, the baby would definitely be alive today. Had the mother had continuous electronic fetal monitoring, the baby would almost certainly be alive today. Had the mother given birth in a hospital, the baby would likely be alive today.
7. Another HBAC: another rupture, another hemorrhage, another baby dies
Let’s see: a homebirth, 2 previous C-sections, a macrosomic baby, and undiagnosed pre-eclampsia. The perfect homebirth candidate!
And look how well it went. The uterus ruptured, the placenta tore away from the uterine wall and he baby died long before she ever got to a hospital. Way to trust birth!
As a bonus, the mother had a massive hemorrhage, extensive abdominal surgery and will be unable to bear any children in the future. Hey, ICAN, are you going to feature this story?
8. Prominent midwife retires after homebirth death
Back in April Brynne Potter, CPM, in her role as a board member of NARM (North American Registry of Midwives) appeared on the Kojo Nnmadi radio show to defend Karen Carr, the midwife who pled guilty to felony charges in connection with the homebirth death of a breech baby. What Potter neglected to mention is that she was on leave from her practice for recently presiding over — you guessed it — the homebirth death of a breech baby.
In the wake of that death, Potter is giving up the practice of midwifery.
9. Third North Carolina homebirth death
The mother is a diabetic (not gestational) who labored at home and ultimately transferred to the hospital after pushing for many hours. The baby was born by C-section, asphyxiated and brain dead, as well as suffering from overwhelming group B strep sepsis. The baby was taken off life support the next day.
10. Mother of 6 dies in the wake of attempted homebirth
The mother posted on homebirth websites and reported that she had already had one successful homebirth after 2 previous C-sections.
In the wake of her death, a friend began soliciting breast milk for her baby:
A beautiful, wonderful, amazing friend of mine passed away on Monday (08/22/11) after giving birth to her sixth child just a day before. She never got to meet her son, as she had lost so much blood by the time he was taken via emergency cesarean section. She tried so hard for this last pregnancy, and continued to nurse her second youngest (nearly 2 now) through it. She was a beautiful, WONDERFUL soul…
Her doula Michelle Fonte had posted a prayer request on August 21:
PLEASE. energy. thoughts. prayers for a very special mama of mine. in the hospital. who needs all of our help. she needs you. really. really.
Unfortunately, she died the next day.
11. Another needless, senseless, utterly predictable, totally preventable homebirth death
The latest needless, senseless, utterly predictable and totally preventable homebirth death is currently being discussed on the Birth Without Fear Facebook Page, which links to the original story and a picture of a beautiful baby who looks to be sleeping but who is actually dead.
I had the most simplest pregnancy, and the healthiest baby boy, decided at 8 months to ditch my OBGYN and go with a midwife and home birth to welcome my son into this world as calming and peacefully as I could. I did chose to go with an unlicensed midwife, as licensing is not required in the state of Oregon, but the greatest mistake of all was not seeing the warning signs for myself. his being my first born I put all my trust and faith into two midwives, who in the end made some bad decisions and proved to be quite negligent. After a full 8 days of labor I delivered my son at home with no heart beat. After all I had done to prepare him for his peaceful arrival, instead of living he rests peacefully….
12. Author of “Perfect Birth Experience” has a dead baby
Canadian homebirth celebrity Annie Bourgault had a twin homebirth. One of them lived and one of them died.
Bourgault describes herself as:
… a reporter who finds evidence based information about birthing. She interviews health professionals, leading experts in childbirth and parents whose work help women feel empowered and fulfilled during pregnancy, birth and motherhood. Sign up for her free report: 7 Steps To The Perfect Birth Experience.
Bourgault was expecting twins, and her “perfect birth experience” did not involve being “fearful of the birth process.”
Pushing Max who was breech was amazing. I could even say it was easy-ish. Even if it wasn’t that easy. It felt like it. When I held him in my arms I kept thinking: “What was the big deal? Why did the hospital refused to let me birth you the way I wanted? Without drugs? Without a c-section? I knew we could do it.”
Then Sam… came out 45 minutes after his little brother. He was in a perfect position: head down. We heard his little heart beating 10 minutes before he came out…everything was fine…seemed fine. While I was pushing him out I heard my midwife say: Oh no! It’s the placenta!” She came in front of me and said: “push your baby out right now!”
… I pushed a baby and a double placenta at the same time…
… I kept saying his name over and over..like a song. I thought if he had a name he couldn’t die. ” … I kissed him, massaged him, loved him with all I had. I believed he was going to be OK.
He wasn’t. He never took a breath.
13. Postdates + long labor + CPM = dead baby
The whole “trust birth” thing continues to work out very poorly for homebirth midwives, the mothers they serve, and most of all the babies who die preventable deaths because of their lack of education and training. Consider the homebirth death that occurred in the Santa Cruz area under the care of “Rebecca, CPM.”
At some point during the 54 hours of labor, the baby stopped getting adequate oxygen. The baby expelled meconium repeatedly, suggesting that she suffered for hours. An electronic fetal monitor would have made it clear that the baby was oxygen deprived, but they didn’t want that, because they were trusting birth. As is all too common at homebirth, the baby died after a long struggle and the CPM not only had no idea that the baby was struggling, but she had no idea that the baby was dead.
To summarize, a postdates mother was allowed to labor for 54 hours with grossly inadequate monitoring of the baby and the baby died a completely preventable death. Why? Because the parents trusted a CPM, an ignorant, undereducated, undertrained, self proclaimed “midwife” who blithely sat by completely clueless while a baby’s life ebbed away.
14. Lisa Barrett presided over a 5th homebirth death
Yes, Lisa Barrett did preside over another homebirth death. The story has just appeared on Adelaide now, aptly titled Inquest midwife Lisa Barrett helped deliver twins, one which later died:
The State Coroner was notified of the death last week of a newborn twin treated at the Women’s and Children’s Hospital.
The Advertiser has learned that birthing advocate Lisa Barrett presented to the WCH with the child’s mother in a taxi.
She had been assisting the mother with a homebirth when complications arose following the delivery of the first child, after which a taxi was called.
15. Kim Mosny presides over homebirth tragedy
Kim wants you to believe that there was no way this could have been prevented.
… Midwives care only for low-risk women, who have healthy life-styles; who do not smoke, drink alcohol, or abuse drugs, and who’s medical status is determined to be healthy, without medical conditions or diseases that would risk them out of care. Thus, there were no other risks that could be determined as causal for this client’s placental abruption. As a result of the abruption, the baby was very quickly deprived of oxygen and he died. He felt no pain. Thankfully, the mother remained stable and did not suffer medical complications herself.
Technically speaking, everything that Mosny wrote may be true. However, she left out some critical details that cast a very different light on the tragedy.
The patient was 42 weeks and 1 day when this stillbirth happened. While the actual precipitating event that led to the baby’s death may not have been preventable, the death itself may have been preventable. The stillbirth rate rises steadily at the end of pregnancy, and 42 weeks is considered the outermost cut-off for induction and delivery of the baby. Had this patient been induced in the hospital before 42 weeks, the outcome would likely have been a healthy baby.
16. Severe IUGR and stillbirth
She planned a homebirth with the same CPM despite her history of a previous C-section, a macrosomic baby, an occult cord prolapse and a postpartum hemorrhage.
At 41 weeks, her daughter died in utero on Thanksgiving day. She was delivered later that evening in the hospital. The baby weighed 5 lbs. 15 oz, suggesting that she had been suffering from intrauterine growth retardation likely due to placental insufficiency.
17. 4th North Carolina homebirth death
The latest homebirth death in NC occurred on December 16. According to the Charlotte Observer:
Just before 8 p.m. Dec. 16, police and paramedics were called to a home on Seamill Road, in a neighborhood near the Catawba River. They discovered the newborn unresponsive.
Charlotte-Mecklenburg police said it appeared complications had occurred after the baby’s mother participated in a water birth – a method of giving birth in a tub of warm water.
Paramedics performed CPR and then took the baby to Carolinas Medical Center, but the infant soon died.
Homicide detectives, who respond to all infant deaths, said they began investigating and determined that two women were in the home at the time of the birth. Police said they were practicing midwifery but did not have the proper license required by state law. Police arrested Mary Stewart Barhite, 43, of Charlotte, and Jacqueline Lynn Proffit, 45, of Indian Trail, on Friday. They are charged with practicing midwifery without a license – a misdemeanor.
*****
These 17 deaths are just the ones that I could confirm; there have been others.
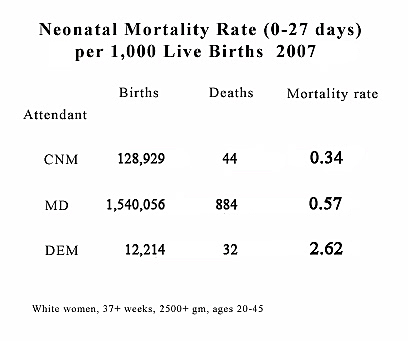
Of note, 13 of these deaths occurred at the hands of American lay midwives and CPMs. There are approximately 10,000 American births attended by non-nurse midwives each year. The death rate for comparable risk hospital birth is 0.4/1000, which means that there should be approximately 4 deaths each year. Instead there have been 13 deaths that I have heard about and confirmed for a death rate that is more than 3X higher than comparable risk hospital birth. The real death rate for homebirths attended by CPMs and other lay midwives is undoubtedly much higher. (Addendum: One death is is a stillbirth, so there were 12 neonatal deaths for a rate 3X higher than comparable risk hospital birth.)
Homebirth with a CPM kills babies. There is no doubt about it. All the state and national statistics confirm this. MANA (Midwives Alliance of North America) is hiding its own death rates because they confirm this. The homebirth deaths of 2011 are yet further confirmation.
How many babies have to die preventable deaths at homebirth before homebirth advocates acknowledge the obvious?