

How do homebirth midwives handle mistakes? They bury them, of course, and a recent study from New Zealand is yet another case in point.
From the title,Planned Place of Birth in New Zealand: Does it Affect Mode of Birth and Intervention Rates Among Low-Risk Women?, to the conclusion, the authors refuse to address the increased neonatal death rate. In fact, the authors go so far as to deliberately obfuscate the increased neonatal death rate at homebirth.
Here’s how the authors represent the findings of their study:
Women planning to give birth in secondary and tertiary hospitals had a higher risk of cesarean section, assisted modes of birth, and intrapartum interventions than similar women planning to give birth at home and in primary units. The risk of emergency cesarean section for women planning to give birth in a tertiary unit was 4.62 (95% CI: 3.66–5.84) times that of a woman planning to give birth in a primary unit. Newborns of women planning to give birth in secondary and tertiary hospitals also had a higher risk of admission to a neonatal intensive care unit (RR: 1.40, 95% CI: 1.05–1.87; RR: 1.78, 95% CI: 1.31–2.42) than women planning to give birth in a primary unit.
Here’s what the authors conclude:
Planned place of birth has a significant influence on mode of birth and rates of intrapartum intervention in childbirth.
Here’s what the authors deliberately tried to hide:
The neonatal death rate in the planned homebirth group was 1.1/1000. The neonatal death rate in the planned hospital birth group was 0.3/1000. In yet another example of a strikingly robust finding, planned homebirth in NZ had more than triple the neonatal death rate of planned hospital birth.
How was the study done?
Data were obtained from the [Midwifery Maternity Provider Organisation (MMPO) database] for a total of 39,677 births. Of these, 16,453 (41.47%) met the study’s low-risk criteria. Of this low-risk group, 11.3 percent were planning to give birth at home, 17.7 percent in a primary unit, 45.5 percent in a secondary level hospital, and 25.4 percent in a tertiary level hospital.
Where did the women ultimately give birth?
Most women gave birth in their planned place of birth; 82.7 percent of those planning a home birth, 90.2 percent planning to give birth in a birth center, 99.8 percent planning to give birth in a secondary hospital, and 99.8 percent planning to give birth in a tertiary hospital actually gave birth in their planned place of birth.
In other words, the transfer rate in the homebirth group was 17.3%; the transfer rate in the birth center group was 9.8%.
The authors are very excited about the difference in intervention rates among these groups, presented in the following table.
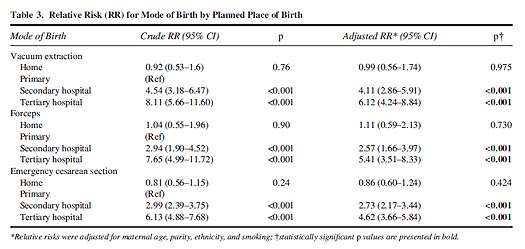
Not surprisingly, the risk of operative vaginal delivery and the risk of emergency cesarean section are much higher in the hospital. The authors do not define “emergency cesarean” but they apparently mean unplanned, not true emergency C-sections.
The authors also looked at secondary outcomes:
… Women planning to give birth in secondary or tertiary level hospitals were also at increased risk of artificial rupture of the membranes, augmentation of labor, pharmacological pain management, episiotomy, and neonatal admission to intensive care when compared with women planning to give birth in primary units. Those planning to give birth at home were at less risk of augmentation of labor, artificial rupture of membranes, pharmacological pain management, episiotomy, and perineal trauma than those planning to give birth in primary units…
So the homebirth group had lower rates of major interventions and the homebirth group had lower rates of minor interventions. How about deaths?
Well, funny you should mention that. There was a little bit of a problem there and the authors made a valiant attempt to hide it.
A total of six neonatal deaths (a death occurring up to 27 days after birth) occurred in the sample, two (0.11%) from women planning a home birth and four (0.15%) from women planning to give birth in the tertiary hospital. No intrapartum, intrauterine deaths were reported.
Hey, the death rates are exactly the same! Wait, what? The authors deliberately used the wrong denominator for calculating the hospital birth death rate?
Indeed they did. They compared the death rate at homebirth with the death rate in tertiary [high risk] facilities, but that’s not what we want to know. We want to know how the death rate at homebirth compares with the death rate at all hospital births, not the death rate at tertiary facilities.
What the authors should have told us was that there were two neonatal deaths (0.11%) among women planning a home birth and four (0.03%) from women planning to give birth in the hospital. In other words, the homebirth death rate was more than triple that of the hospital birth death rate. Oops!
The authors of this paper should be ashamed of themselves. They didn’t want anyone to know that homebirth had triple the neonatal death rate of hospital birth, so they deliberately obscured it by using the wrong denominator in their calculations.
The authors brazenly assert that no differences for planned place of birth were noted. That is simply a lie.
Homebirth in New Zealand has triple the neonatal death rate of hospital birth. The finding of lower intervention rates in the homebirth group is nothing to celebrate when more babies died as a result.
