
Believing that vaginal birth is an achievement depends on a fundamental misunderstanding about why some babies fit and others do not. Women have NO control over whether a baby is going to fit, therefore they should not be taking any credit if the baby does fit and they should not be taking any blame if the baby does not fit.
In other words, the claim that vaginal birth is an “achievement” or “empowering” or worthy of praise makes as much sense as believing your eye color is an achievement or empowering or worthy of praise. You have to be pretty desperate for positive attention to take credit for bodily attributes that are beyond anyone’s control.
Let’s leave aside for the moment the issue of whether the baby can tolerate labor and look only at the factors that determine whether the skull of the baby will be able to pass through the bones of the mother’s pelvis. Four major factors are involved: pelvis, passenger, fetal position and power. Women can control NONE of them.
I’ve written about the pelvis and the passenger (fetus) before:
Most people imagine that the pelvis is like a hoop that the baby’s head must pass through, and indeed doctors often talk about it that way. However, the reality is far more complicated. The pelvis is a bony passage with an inlet and an outlet having different dimensions and a multiple bony protuberances jutting out at various places and at multiple angles. The baby’s head does not pass through like a ball going through a hoop. The baby’s head must negotiate the bony tube that is the pelvis, twisting this way and that to make it through…
There are bony protuberances that jut into the pelvis from either side (the ischial spines) and the bottom of the sacrum and the coccyx, located in the back of the pelvis, jut forward. How does the baby negotiate these obstacles? During labor, the dimension of the baby’s head occupies the largest dimension of the mother’s pelvis. But because of the multiple obstacles, the largest part of the mother’s pelvis is different from top to middle to bottom. Therefore, the baby is forced to twist and turn its head in order to fit.
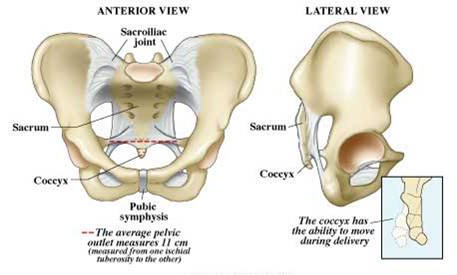
If the pelvic inlet is toot small the baby’s head may never even drop into the pelvis. If the ischial spines stick too far into the pelvis,the head the head will not be able to get past them. If the sacrum and coccyx are angled too far forward they may stop the head from going farther.
It isn’t a matter of the absolute dimensions of the pelvis, but the dimensions relative to the individual baby. Almost all women can vaginally deliver a small baby, but a big baby is another matter entirely. The claims of natural childbirth and homebirth advocates that “a mother cannot grow a baby too big for her pelvis” is simply made up. The size of the mother’s pelvis is determined by her genes and the size of the baby is determined by her partner’s genes as well. His genetic contribution may lead to a large baby and that isn’t going to change simply because the mother’s pelvis is small.
Over time, babies have evolved so that the bones of the skull are not fused and can slide over each other, reducing the diameter of the head. This is called “molding” and accounts for the typical conehead of the newborn. But there is a limit to the amount of molding that the head can undergo and ultimately, the baby may not fit.
That’s pelvis and passenger. What about position? The optimal position for a baby to enter the pelvis is head first, spine facing the mother’s front. This position is known as occiput anterior. Babies don’t always cooperate. If the head is in anything other than the ideal position the fit will be even tighter. That’s why babies in the OP position (facing frontwards) and babies with asynclitic heads (the head titled to one side) are much more difficult to deliver vaginally. Their heads no longer in the smallest possible diameter. It’s like trying to put on a turtleneck face first of over your ear instead of starting from the back of your head. It’s much more difficult.
The final factor is power. Even if the baby is small enough to fit through the pelvis, it won’t go through unless the uterus is pushing against the baby with a sufficient amount of force to counter the resistance of the soft tissue and pelvic bones. The power is the strength, duration and frequency of uterine contractions. Any or all of these can be insufficient to push the baby through the pelvis. That’s where pitocin comes in. Inadequate contractions can be strengthened by pitocin, and the frequency and duration of contractions can be increased. Many women and babies who would have died before the advent of pitocin for labor augmentation have smooth uncomplicated labors once pitocin is given to the mother.
What can the mother do about these factors? Absolutely nothing. She cannot increase the diameter of her pelvic inlet, change the shape of her ischial spines or decrease the angle of her sacrum. She can do nothing about the size of the baby. She can do nothing about the position of the baby. She can do nothing about the power of her uterus.
The only thing a woman can do is to continue with a protracted labor and hope that the baby will eventually fit through. This is where we have to return to the issue of whether the baby can tolerate labor.
Labor is stressful for the baby. Every contraction cuts off blood flow to the placenta. Therefore, the baby is essentially “holding its breath” with every contraction. The placenta is supposed to transfer enough oxygen between contractions so that the baby can tolerate being deprived of oxygen for a minute or more every two minutes. The oxygen transfer capacity of the placenta can be compromised by a variety of factors including high blood pressure, post dates, or an undiagnosed deficiency in the placenta itself. Even a healthy baby with a healthy placenta may be unable to withstand labor indefinitely. The longer the labor lasts, the greater the risk to the baby.
Strictly speaking, the baby is either going to fit or not going to fit and there’s nothing the mother can do about it. If the baby is not going to fit she will eventually have to consent to a C-section or she will ultimately die.
If the problem is poor uterine power, the baby may eventually come through after a very long labor, putting the baby at risk of distress and the mother at risk of postpartum hemorrhage. Treatment with pitocin when the labor is diagnosed as protracted will take hours off the labor, with benefits to both mother and baby. Refusing pitocin can paradoxically increase the need for a C-section by increasing the length of labor until the baby can no longer tolerate it, or until an infection develops or some other complication occurs.
Yes, it is true that a baby born vaginally after a multi-day labor was always capable of fitting and might have been delivered by C-section “unnecessarily” but the corollary is that the baby that ultimately fits may sustain damage from oxygen deprivation during the prolonged labor.
Either way, vaginal birth is not an achievement. If the four factors are not properly aligned, the baby is not coming out through the vagina no matter what. The only issue is how much stress the mother is willing to expose the baby to before she acknowledges reality.