
On it’s face, homebirth advocacy, makes no sense. Anyone with even a modicum of knowledge of science and statistics, let alone a basic knowledge of history, knows that childbirth is inherently dangerous, that life threatening emergencies can occur without warning, and that giving birth at home leads to preventable perinatal deaths.
Nearly every day there is another example in the media or on homebirth blogs and message boards.
Today’s iteration is the completely preventable death of Joseph Thurgood, who died because his mother chose to attempt a VBA2C at home, ending in the exact complication doctors warned her about: her uterus ruptured.
The Coroner’s Court was told that the midwife, Fiona Hallinan, is guilty of a gross breach of her duties. And, of course, the mother “educated” herself about homebirth:
A “high risk” pregnant woman who mistrusted doctors and did her own medical research was repeatedly warned of the dangers of a home birth, an inquest on her baby heard yesterday.
Kate Thurgood had delivered two children by caesarean section and was “determined” to have a child naturally and at home.
After doing her own research on the internet she dismissed concerns raised by doctors about the position of her baby and complications raised by her earlier caesareans.
“(She was told) she should not labour or deliver at home and she should have an elective caesarean section at hospital,” Dr Paul Halley, of Southern Health, told the Coroner’s Court.
Mrs Thurgood did her own web-based research on the risks, questioned several doctors’ advice, and sought out midwife Fiona Hallinan to help her deliver the child at home, the inquest heard.
So why do women like Kate Thurgood choose homebirth? I would argue that its real appeal is that homebirth advocacy, like all pseudoscience, flatters the ignorant.
In the real world, the majority of people recognize that science and statistics are difficult, specialized subjects and that medicine, including obstetrics, requires years of study and years of experience to master. In the world of pseudoscience, there is no need for hard work. All you need to do to be qualified to argue with your doctor, advise anonymous people on message boards, and set up your own website to “educate” others is to do “research” on the web.
Don’t worry, “research” on the web is not nearly as difficult as it sounds. It’s not as if you are expected to actually READ any scientific papers. Merely cutting and pasting their titles and abstracts is enough. Then you cherry pick the statements that you like from relevant professional organizations, while simultaneously ignoring any statements that you don’t like. And finally, you rely heavily on the Dunning-Krueger effect.
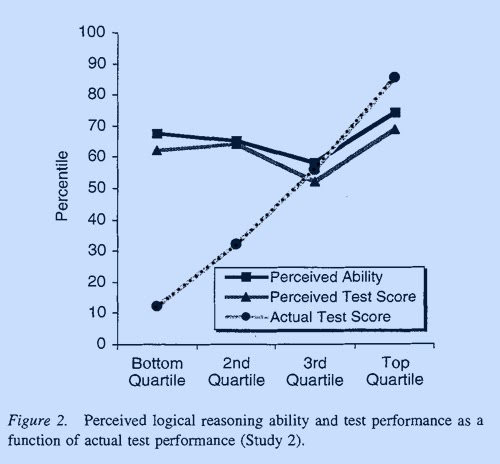
What’s the Dunning-Krueger effect? The classic paper on this phenomenon is Unskilled and Unaware of It: How Difficulties in Recognizing One’s Own Incompetence Lead to Inflated Self-Assessments by Kruger and Dunning published in Journal of Personality and Social Psychology in 1999. The paper reports on a variety of experiments that were used to evaluate individuals’ actual performance compared to predicted performance.
As the chart below demonstrates, those that knew the least about the subjects under discussion thought that they knew the most. In other words, those who knew the least were also the least capable in understanding how little they knew.
Dunning and Krueger explain:
… [I]ncompetent individuals may be unable to take full advantage of one particular kind of feedback: social comparison. One of the ways people gain insight into their own competence is by watching the behavior of others… However, [our study] showed that incompetent individuals are unable to take full advantage of such opportunities. Compared with their more expert peers, they were less able to spot competence when they saw it, and as a consequence, were less able to learn that their ability estimates were incorrect.
Homebirth advocacy leverages the Dunning-Krueger effect to flatter the ignorant into believing that they are educated, as if being educated were merely a matter of defying authority and reading websites and books written by other laypeople.
The Dunning-Krueger effect is pretty powerful. Hence the perverse persistence of those who parachute into this blog to “educate” me. They are impervious to reason. Point out to them that they have not read the scientific literature they are quoting and they are unabashed. Point out to them that they cherry pick the statements of professional organizations, brandishing those they like and ignoring everything else and they are unembarrassed. Point out to them that there are specialists with years of training and experience, people who actually DO the research on childbirth, who have reached conclusions the opposite of theirs and they are unmoved. Why? Because to acknowledge the relevance of actually reading the literature, and following the recommendations of professional organizations and clinicians undercuts their insistence that they are “educated.”
Homebirth advocates, like advocates of vaccine rejection and other forms of pseudoscience, cling desperately to their beliefs in the face of both evidence and logic, not merely because they need to believe the foolishness that they believe. At its heart, the promotion of pseudoscience gives the ignorant the delusion of being educated without any of the hard work that really being educated requires. And that flattering delusion of being knowledgeable, when in reality they are ignorant, is too precious to give up, even for something as important as the life of your own baby.