

The American Academy of Pediatrics has issued a policy statement on homebirth. It has been getting a lot of press, but most mainstream media sources seemed to have missed its true significance. NBCnews.com, Time, The Huffington Post and The Atlantic, among others, have highlighted the fact that the AAP issued guidelines at all, and haven’t noticed that most American homebirths fail to meet virtually all the guidelines. Rather than supporting homebirth as it currently exists, the AAP is actually condemning it.
The policy statement starts by stating the obvious: the homebirth is not as safe as hospital birth.
The American Academy of Pediatrics concurs with the recent statement of the American College of Obstetricians and Gynecologists affirming that hospitals and birthing centers are the safest settings for birth in the United States …
But for those women who would rather choose the less safe option, the AAP offers guidelines to minimized the increased risk, summarized in the following chart.
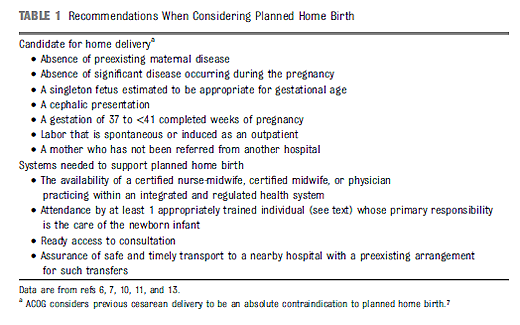
They can be summarized as follows:
No homebirth midwives (only certified nurse midwives are safe practitioners.)
No twins.
No breech.
No VBAC.
No postdates.
No macrosomic babies.
No pregnancy complications of any kind.
Contrary to the prattling of homebirth midwives, NONE of those issues are variations of normal; ALL are complications.
Once all complications are excluded, there are still additional safety steps that should be taken:
The midwife must be practicing within the medical system.
A second midwife (or pediatrician) must be available to care for only the baby.
Physician backup.
A PRE-EXISTING arrangement with a hospital for transfer.
In other words:
Don’t undertake homebirth when there is ANY increased risk of complications. Don’t undertake homebirth without 2 midwives, integrated into the health care system, who have physician back up and a pre-existing transfer arrangement with a nearby hospital.
The AAP recognizes that childbirth is dangerous, complications are common, any risk factors mean that the mother is not an appropriate candidate, and systems must be in place for the additional complications that will inevitably occur.
The AAP guidelines can be summed up very simply:
Don’t trust birth!
Even leaving aside their inadequate education and training, American homebirth midwives (CPMs, LMs, DEMS and lay midwives) routinely violate every guideline set forth by the AAP. That’s why they are unsafe practitioners and why the CPM credential must be abolished.
Mainstream media sources seemed to have missed the central point of the AAP guidelines, homebirth as it is currently practiced in the US not merely less safe than the hospital, it is unsafe.
