

Lana Muniz, PhD has prepared a fabulous resource on state midwifery laws and their impact on homebirth mortality rates.
Muniz wanted to know whether stricter regulation of homebirth midwives leads to better outcomes.
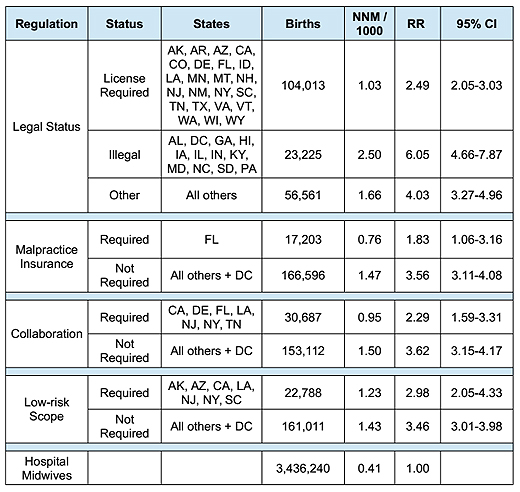
Using the CDC Wonder website, U.S. neonatal mortality rates (NNM) are examined for term, singleton births attended by non-nurse midwives in out-of-hospital settings. States are grouped by regulatory status, and NNM of those groups are compared to assess whether state midwifery laws have an impact on out-of-hospital birth mortality.
Not surprisingly, more regulation of homebirth midwives and greater adherence to the regulations leads to lower risk of perinatal death at homebirth.
States which require midwives to be licensed have a 30% reduction in NNM below the national average. States which also require malpractice insurance (only Florida during the study period) have a 50% reduction in NNM, though this result does not quite reach statistical significance at the 5% level.
The impact of requiring collaboration or a low-risk scope is unclear due to small sample size. The RR for scope has a large confidence interval, and the collaboration study is highly correlated with the malpractice insurance study; Florida births comprise over half the collaboration study group. Thus, there is insufficient data to conclude whether collaboration and low-risk scope have an impact on NNM.
However, it is clear that mandatory malpractice insurance is the most important driver of safer outcomes at out-of-hospital births, for it cuts neonatal mortality in half. Requiring malpractice insurance and collaboration did not appear to restrict access to out-of-hospital births, since nearly 10% of out-of-hospital births under study were in Florida. However, even with these regulations, the mortality rate in Florida (RR: 1.83) is almost double that of births to hospital midwives.
You can find the whole report below:
[gview file=”http://www.skepticalob.com/wp-content/uploads/2014/11/Do-State-Midwifery-Laws-Matter-v1.pdf”]
You can download the entire report here.
Kudos to Muniz for the massive amount of work that went into this and for the valuable information that resulted. This will help women make better decisions about the risks of homebirth.
