

The new Lamaze poster on epidurals raises some existential questions for me and perhaps my readers could help me out.
Which of the many ethical violations that Lamaze has committed within the poster are the worst?
Is it the lying about facts?
Is it the lying about judgment?
Or is it the way they treat their followers with utter contempt, imagining that they are stupid enough to swallow anything that the liars at Lamaze dish out?
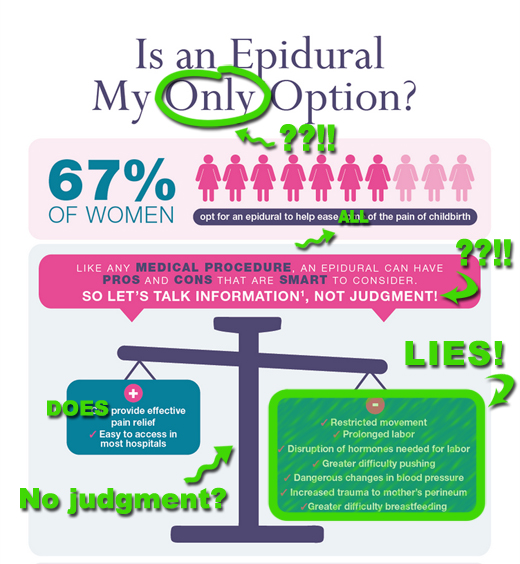
Here’s my annotated version of the top of the poster to help you out:
Personally, I’m leaning toward the bald faced lies as the worst ethical violation.
It doesn’t matter to the folks at Lamaze what the scientific evidence shows. They are entirely evidence resistant. They are a business that depends on demonizing epidurals and they apparently see no problem with lying if that’s what promotes profits. Consider the plethora of lies above. In direct contrast to what Lamaze claims:
1. The fact that epidurals restrict movement has no impact on labor.
2. The “prolongation” of labor is measured in minutes and has no impact on anything.
3. There is NO DISRUPTION of hormones needed for labor. That is pure invention on the part of the liars at Lamaze.
4. There are no “dangerous” changes in blood pressure. Temporary drops in blood pressure are easily reversed and have no harmful effects.
5. There is NO EVIDENCE that epidurals cause trauma to the perineum.
6. There is NO EVIDENCE that epidurals cause difficulty breastfeeding.
The liars at Lamaze are batting 1000. Six claims and all six are lies. Way to go, Lamaze liars!
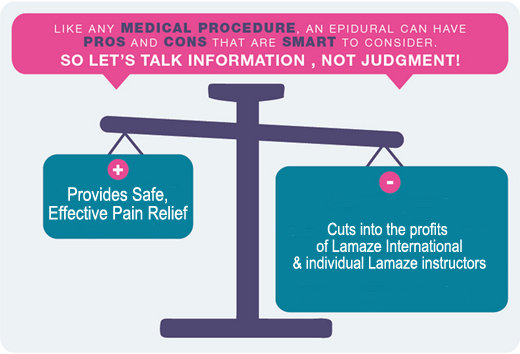
You know what the biggest risk of epidurals is? Epidurals decrease Lamaze profits!
That’s right. Lamaze is a business and it makes it money in two ways: it licenses infant toys (I kid you not) and it charges certification fees for Lamaze educators. Because Lamaze has chosen to indoctrinate its educators with bald faced lies about epidurals, epidurals themselves pose a tremendous economic threat. Who needs an educators to lie to women about epidurals if they find out that epidurals are SAFE, HIGHLY EFFECTIVE, have MINIMAL SIDE EFFECTS, TRIVIAL IMPACT ON LABOR, and NO EFFECT ON BREASTFEEDING? Apparently no one, hence the need for lying at Lamaze.
I must say that the Sanctimommy lie about no judgment is a nice touch. They are so not judging you even if you are benighted enough to believe that epidurals are the only way to relieve pain in labor (they are, of course, the only EFFECTIVE way to relieve pain in labor), even if you think epidurals relieve pain, and even if you are weak and lazy enough to pick the con side of the scale. Got to love that subliminal sanctimony of portraying the choice as the balancing scale, and weighing down the con side with lies.
Even so, I think you could make a good argument for the fact that the greatest ethical malfeasance of the liars at Lamaze is the absolute contempt with which they treat their followers. They figure that their followers are stupid enough to get their information about epidurals from people who only make money by demonizing epidurals. It’s like getting your information on renewable energy from oil companies. They believe their followers are gullible enough that they can lie with abandon and no one will either know or care. Not to mention that the liars at Lamaze apparently think any amount of women suffering any amount of agonizing pain is fine when balanced against the profits of the Lamaze itself.
Keeping that in mind, I’ve helpfully amended the Lamaze balance scale:
In conclusion, let me reassure the liars at Lamaze that I wrote this post about their lies with no judgment, exactly the same way that they designed their poster!
