

To the Editors of the British Journal of Obstetrics and Gynecology,
Thank you so much for response to my tweets about the recent publication of Safe for Whom? by Melissa Cheyney et al. and your suggestion to submit a Letter to the Editor.

The format for Letters to the Editor is too restrictive, so I decided to share my concerns in this open letter.
Simply put, dear Editors, what were you thinking?
[pullquote align=”right” color=”#dd2332″]Melissa Cheyney has lied, denied, decried and defied efforts to inform the public of the hideous death toll at homebirth.[/pullquote]
Did you actually solicit an opinion piece from a LAY midwife, indeed the lay midwife who has single-handedly done more to hide the growing toll of tiny bodies of babies who succumb to American homebirth than anyone else? Melissa Cheyney has lied, denied, decried and defied efforts to inform the public of the hideous death toll at homebirth.
Did you know that Cheyney, like all American “certified professional midwives” (CPMs) is grossly undereducated, grossly undertrained and fails to meet the standards for ALL other midwives in the industrialized world?
Did you know that the CPM credential was fabricated from whole cloth by lay people who couldn’t be bothered to get a real midwifery degree, but wanted to hijack the excellent reputation of American certified nurse midwives by awarding themselves similar letters after their names?
It appears that you are unaware that Cheyney, in her role as the Chair of the Oregon Board of Direct Entry Midwifery, steadfastly REFUSED to release the homebirth mortality rates in her possession for fear that regulatory authorities might wish to investigate the death rate and discipline the midwives involved in the deaths:
Cheyney explained … due to some state regulatory boards having very hostile relationships with midwives, the quality and quantity of data submitted might be adversely affected if regulatory authorities were provided access.
The state of Oregon subsequently hired Judith Rooks, CNM, MPH, a known supporter of homebirth, to calculate the Oregon homebirth death rate in 2012. Rooks presented her findings in this chart:
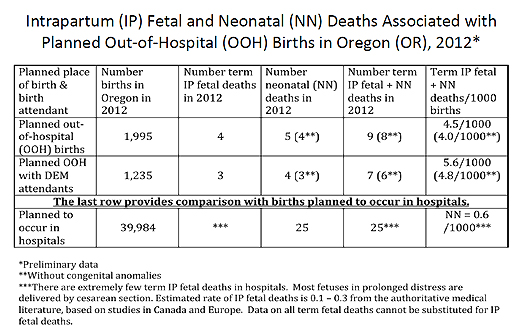
Rooks regretfully acknowledged:
Note that the total mortality rate for births planned to be attended by direct-entry midwives is 6-8 times higher than the rate for births planned to be attended in hospitals. The data for hospitals does not exclude deaths caused by congenital abnormalities.
Many women have been told that OOH births are as safe or safer than births in hospitals…
But out-of-hospital births are not as safe as births in hospitals in Oregon, where many of them are attended by birth attendants who have not completed an educational curriculum designed to provide all the knowledge, skills and judgment needed by midwives who practice in any setting.
These were the statistics that Melissa Cheyney tried to hide.
Did you know that in her role at Director of Research for the Midwives Alliance of North America (MANA), the trade union that represents homebirth midwives, Cheyney REFUSED for 5 years to release the mortality rates from a MANA survey of nearly 20,000 homebirths from 2004-2009, hiding them until 2014 when the pressure became too great.
Undoubtedly you know that Cheyney ultimate published the results in Outcomes of Care for 16,924 Planned Home Births in the United States: The Midwives Alliance of North America Statistics Project, 2004 to 2009. Did you read the paper? If you had, you would have found that comparing Cheyney’s death rate at homebirth of 2.06/1000 with the CDC death rate for low risk white women (ages 20-44, at term, with babies that are not growth restricted) of 0.38, we find that homebirth has a death rate 5.5X higher than hospital birth. In other words, the death rate at homebirth is 450% higher than comparable risk hospital birth.
Moreover, the death rates in certain subgroups were astronomical:
(5 fetal/neonatal deaths in 222 breech presentations), TOLAC (5 out of 1052), multiple gestation (one out of 120), and maternal pregnancy-induced comorbidities (GDM: 2 out of 131;
preeclampsia: one out of 28
You can also be sure that the authors understood that their data showed that homebirth has a horrifically high death rate, because they try to hide the number of deaths for the past 5 years, released the data only under pressure, and then proceeded to draw a conclusion entirely at odds with what their own data showed. In addition, you can also conclude that homebirth is NEVER appropriate for breech, twins or VBAC. Finally, you come away from the paper with the horrifying realization that MANA has absolutely no idea what its own members are doing. There is no systematic attempt to determine if they are safe practitioners.
Is it any wonder then that Cheyney, who has spent years hiding the death toll at homebirth in her own state and across the country dismisses even the idea of homebirth safety by asking “safe for whom”?
And is it any wonder that Cheyney tries to reframe the conversation to ignore the death rate altogether:
Let us move beyond this polarising debate on whether homebirth is safe …
It was grossly inappropriate to solicit a commentary on homebirth safety from Melissa Cheyney, a lay midwife who has spent her career lying about the death toll of American homebirth.
BJOG should retract Cheyney’s latest effort at obfuscation and apologize to its readers for soliciting her opinion in the first place.
Sincerely,
Amy B. Tuteur, MD
