

Lactation consultants and organizations tell new mothers that the average size of a newborn baby’s stomach is only a teaspoon (5 cc). That’s supposed to ease their minds when their newborns are screaming in hunger and they can tell that they are producing very little colostrum or milk.
There’s just one problem. It’s not true.
Nevertheless, that lie has been enshrined in a variety of products designed to hammer home the lie to lactation consultants, nurses and new mothers that infants need far less to eat than they really do.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]The average size of the newborn stomach on day 1 is NOT 5-7 cc but 20 cc or more.[/pullquote]
Lactation consultant Christy Jo Hendricks is one of the leading purveyors of products that promote the lie and she’s very upset that the Fed Is Best Foundation is working hard to debunk that lie.
Here is the product that Hendricks sells, a lanyard that supposedly illustrates the size of the newborn stomach on day one.

It’s accompanied by a card that contains 3 sentences, all of them lies.
The biggest lie is that the capacity of the newborn stomach is only 5-7 ml.
Here’s what the scientific evidence actually shows:
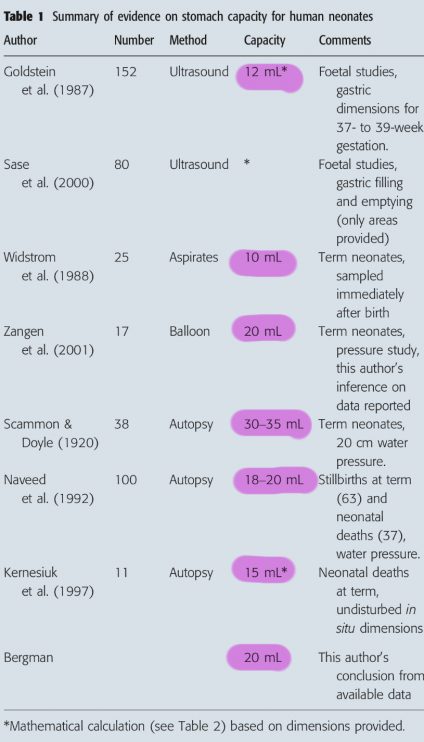
The chart comes from a literature review published in Acta Pediatrica in 2013. You can see that the average stomach size was found to be anywhere from double to nearly quintuple the size quoted by lactation consultants.
Why is there such a big discrepancy? The problem lies in the nomenclature.
The lactivist claim is based on a study from 1920 by Scammon and Doyle. In that study the authors found that the average PHYSIOLOGIC capacity of the newborn stomach is 5-7 cc. but that’s a misuse of the term “capacity.” It’s actually the size of the average infant MEAL as measured by weighing the baby before and after breastfeeding with mothers allowed to breastfeed only 5 time per day. It has nothing to do with the ANATOMIC capacity of the stomach itself.
The anatomic capacity of the stomach is the amount that the stomach can hold during a meal without becoming distended. According to Scammon and Doyle, the ANATOMIC capacity of the stomach at birth is 33 cc. If you look carefully at the chart from the literature review, you will see that Scammon and Doyle report the largest anatomic capacity of any of the papers.
So the average size of the newborn stomach is NOT 5-7 cc but closer to 20 cc, rising dramatically over the first first days. And some babies need every one of those 20 cc per feeding and more!
The Fed Is Best Foundation has filed a complaint with the Consumer Product Safety Commission alleging that the lanyard is based on claims that are factually false and can lead to infant harm.
Dr. Christie Castillo-Hegyi wrote:
“The lactation lanyard and keychain are visual tools used to convince mothers that their newborns are not in need of supplemental feeding. It claims a newborn stomach size of 5-7 mL when in fact the scientific data has shown it is 20 mL. This is leading to dangerous newborn starvation and brain injury…”
How does Hendricks respond?
I know my product is well-respected by professionals and health organizations. I know it contains sound advice, backed by science. Unfortunately, I fell compelled to to respond now because a misled individual has gone to great lengths to discredit my work and the evidence behind it… I am sharing the Open Letter I sent in response … Let’s end her tirade once and for all. Let’s call out those who pretend to support breastfeeding but try to sabotage its success. Let’s expose lies and half-truth.We cannot embrace “alternative truths” when it comes to infant feeding and public health. There is so much more I could say, but for now I will share my response to an invalid complaint about a powerful visual and important teaching tool that is empowering moms around the world.
But you can’t empower women with a lie and Hendricks’ product is based on a serious misunderstanding of a paper from 1920.
In Hendricks’ defense, I doubt that she has ever read the Scammon and Doyle paper. She was taught the lie by other lactivists who did read it and either didn’t understand what they read or chose to lie about what they read.
Why would they lie? For the exact reason that Dr. Castillo-Hegyi noted. It is an effort to prevent women whose babies are screaming from hunger to supplement with formula.
Lactivists don’t merely fetishize breastmilk as some sort of magic elixir, they also fetishize exclusivity. They suggest or even claim that “one bottle” of formula can ruin the breastfeeding relationship and the infant gut microbiome. Neither is true. Indeed no less an authority that Alison Stuebe, MD of the Academy of Breastfeeding Medicine acknowledges:
…a substantial proportion of infants born in the US require supplementation. Delayed onset of lactogenesis is common, affecting 44% of first-time mothers in one study, and 1/3 of these infants lost >10% of their birth weight. This suggests that 15% of infants — about 1 in 7 breastfed babies — will have an indication for supplementation.
Other scientific evidence demonstrates that judicious early formula supplementation not only DOESN’T harm the breastfeeding relationship, but can actually IMPROVE it.
Hungry babies are suffering babies. Most mothers understand that instinctively and want to ease their babies’ pain by supplementing. Lactivists prefer to let babies scream. Instead lactivists falsely reassure mothers with products that graphically represent a believe a lie.
That’s not merely wrong and dangerous to infant health; it is insupportably cruel.
