

Melissa Cheyney is the Donald Trump of homebirth midwifery. Both think they can trick their followers and get away with it.
Trump has nothing on Cheyney and the Midwives Alliance of North America (MANA) when it comes to treating their followers with contempt. They appear to think that their followers are both stupid and gullible.
The only thing that is more amazing than their contempt is the fact that it is justified. It doesn’t matter how often Cheyney and MANA (or Trump) obfuscate, their followers slurp it up and then lick the floor looking for more.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]In a more than 3000 word piece ostensibly explaining the relative risks of homebirth, Melissa Cheyney refuses to tell women the actual risks.[/pullquote]
Last week I wrote Cheyney and MANA have finally acknowledged the hideous homebirth death rates that they’ve been hiding for years. The paper is Perspectives on risk: Assessment of risk profiles and outcomes among women planning community birth in the United States published in Birth: Issues in Perinatal Care, the journal owned by Lamaze International.
How hideous are they?
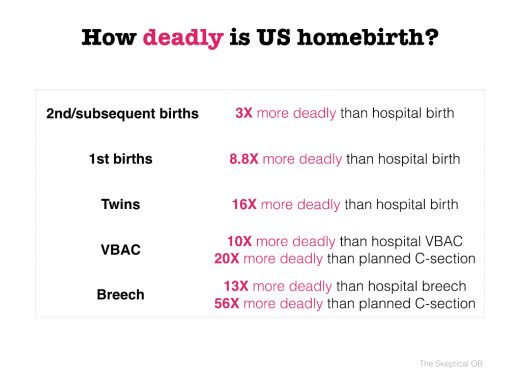
As you can see, in every category — with risks or without — homebirth increases the risk of fetal/neonatal death substantially and often enormously.
Even uncomplicated births to women who have given birth before are 3X more deadly than hospital birth; first births are 8.8X more deadly. It only gets worse from there, culminating in breech homebirths that are 56X more deadly than a planned C-section.
The REAL risks are almost certainly higher because these risks are based on a small subset of MANA members who voluntarily reported their outcomes.
So Cheyney and MANA have publicly acknowledged their hideous death rates, but — and this is the truly astounding part — they have so little respect for the intelligence of homebirth advocates that they think they can hide these death rates from them.
MANA has published Understanding Relative Risks In The Community Birth Setting: An Interview With Researcher Melissa Cheyney. There is not a single number in the piece. In a more than 3000 word piece ostensibly about the relative risks of homebirth, Melissa Cheyney refuses to tell women the actual risks.
Instead, she attempts to baffle them with bullshit.
Following the tactics of Trump, the piece starts with a brazen effort at misdirection:
Community birth (planned home and birth center births) has been demonstrated to be a safe option for low-risk women.
Yes, but NEVER in the US.
There has never been a single study — not even one — that has showed American homebirth to be as safe as comparable risk hospital birth.
According to Cheyney:
We started with the premise that given the larger literature on planned home and birth center births with trained midwives in high-resource countries, home birth clearly can be safe and for some outcomes safer than hospital births for a certain segment of the population. The Dutch, UK, and Canadian studies have clearly shown us this.
That sounds so familiar. It’s almost exactly what I wrote in my New York Times Op-Ed on homebirth Why is American Home Birth So Dangerous.
…[T]here are places in the world where home birth is relatively safe, like the Netherlands, where it is popular at 16 percent of births. And in Canada, where it appears safest of all, several studies have demonstrated that in carefully selected populations, there is no difference between the number of babies who die at home or in the hospital.
In contrast, home birth in the United States is dangerous…
According to Cheyney:
This caused us to question whether we were asking the right questions. Instead of asking, is home birth safe?, we argued that we should be asking, safe for whom?, under what circumstances?, and using whose definition of safe? This study was born out of a commitment to maternal autonomy and informed, shared decision making.
A commitment to informed decision making? How can American women be informed if Cheyney refuses to tell them the actual risks?
Instead:
I would group findings into three categories.
For example:
…[T]here is a third category, which was associated with much higher than anticipated fetal and neonatal mortality and morbidity: women presenting with a breech infant, multiparous women with a history of cesarean but no vaginal birth, and preeclampsia. The breech and preeclampsia findings were not surprising to us, but one of the outcomes we are really grappling with is the risk associated with a labor after cesarean in the community setting when there has been no previous vaginal birth. That is higher risk than we anticipated going into the study.
How much higher? Cheyney won’t say and then offers this:
The practitioner will always need to nuance these findings in their discussions with an individual family. Practitioners can begin by giving families a broad sense of the risk landscape. But then the conversation will have to narrow back in, not only to the mother’s individual risk profile, but also to her value system. It is her body, and until the baby is born, she has full autonomy in decision making. She will need to make choices about her care that fit with her worldview and her value system, because she is the one who will live in that body and raise that baby afterwards.
But how can she make an informed decision if she doesn’t know the actual risks?
My favorite quote, though, is this one:
…[W]hat studies like this do is they offer us the opportunity to be self-critical and reflective. They enable us to turn the lens inward and look at our practice as midwives and say, “Where do we need to improve?”
That’s hilarious — or it would be if American homebirth midwives weren’t presiding over so many deaths.
Cheyney’s study shows beyond any doubt that American homebirth midwives are grossly undereducated, undertrained and deadly. American homebirth is not safe and can never be safe until we abolish the second, inferior class of midwives known certified professional midwives (CPMs). We must mandate that — as in The Netherlands, the UK and Canada — no one should be allowed to call herself a midwife unless she meets the international standards of midwifery.
Only the stupid and the gullible could draw any other conclusion. So the only question that remains is whether American homebirth advocates are that stupid and that gullible.
