

We are arguably living in a golden age of medical science. The great infectious scourges of history — smallpox, diphtheria, polio — have been nearly vanquished by vaccines. Previously deadly infections like appendicitis can be cured with surgery. Cancer and heart disease are yielding their secrets and conditions once thought to be due to sorcery or divine will — from epilepsy to infertility — are now understood and treated. Yet a large swathe of the American population is gullible enough to believe in and spend their money on quackery.
Who believes in quackery and why?
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Believers in quackery are easy marks for unscrupulous marketing messages that are tailored to appeal to their egos for the purpose of draining their wallets.[/pullquote]
In The appeal of medical quackery: A rhetorical analysis, pharmacists Widder and Anderson seek to answer these questions.
Quackery is not new.
From patent medications and nostrums to super-foods and miracle supplements, medical fraud, often referred to as “quackery,” has historically been a pressing and emotionally charged issue for health care professionals. Much like today, historical analysis of 18th century English quackery shows that those making dubious medical claims excelled at 3 things: taking advantage of new market opportunities, building a brand name, and advertising their product.
Who is susceptible to being tricked by quackery?
Overall, the typical CAM [complementary and alternative medicine] user tends to be female, middle aged, and college-educated, with lower perceived health and a higher level of spirituality (seeking answers and understanding to ultimate questions regarding life and its meaning and relationship with the sacred)…
That’s an accurate description of aficionados of quacktress Gwyneth Paltrow, “holistic” psychiatrist Kelly Brogan, herb and supplement peddler Aviva Romm, MD and their ilk.
The authors explain that the typical quack marketing plan is based on four straw-man metaphors:
Profit-mongering “Big Pharma”
The doctor as a deity
Illness as war
The body as a machine
They offer one of the best explications of quack philosophy that I have read.
The metaphors used by alternative medicine amplify genuine critiques of the medical community to extremes, attacking the ethos of modern medicine and its practitioners while moralizing the healing process and dichotomizing medical treatment. In this dichotomy, modern medicine is a cold, disjointed, toxic, “evil” and unnatural force of technology in contrast to a more natural, holistic, pure, good, and balance-driven force for unity that seeks to create conditions of health instead of merely treating specific pathologies. Through all of these arguments, alternative medicine relies on the pathos of anecdotal evidence to prove its efficacy, reinforcing to patients that they know their body better than any medical professional and that they should be treated as an individual and as an equal in the healing process.
To a large extent, as I’ve written in the past, doubt is the primary product of all quacks, specifically doubt about modern medicine and doubt about physicians.
Doubt about modern medicine:
Anything not seen as natural, from vaccines to antibiotics, is Big Pharma’s attempt to accumulate wealth at the expense of the unsuspecting public. Thus, the alternative medicine movement undermines the ethos of Western medicine and establishes a distrust of “unnatural” treatments. Health care has been compared to a “medical market,” where all practitioners “bid” for the trust of their patients. This establishes an ethos attack that sets up modern medicine as a conniving profit center, with the friendlier, seemingly straightforward, natural approach of alternative medicine standing in stark contrast.
Doubt about physicians:
In the “doctor as god” metaphor, alternative medicine … create[s] a perception that Western medical professionals think they know more about their patient’s body and how to heal it than the patient does… This is especially designed to rub against the beliefs of an educated, spiritual audience accustomed to seeking the answers to their own questions, and making educated decisions based on those answers. Once this straw-man has been set up, alternative medicine is able to offer a more egalitarian relationship between a patient and practitioner, emphasizing that a patient knows their own body far better than any physician, and therefore is an integral part of the healing decision process…
The authors also address the other two strawman arguments.
Illness as war:
…[I]llness is the enemy, and practitioners are soldiers fighting for the victim. While this metaphor has been used by modern health care, CAM proponents amplify the metaphor, and then attack that amplification. Alternative medicine proponents … caution that medications, like weapons, can be dangerous and backfire on the user, causing harm or provoking more aggressive tactics from the “enemy.” Then, they offer an alternative by stating that pain is not something to fight, but a messenger and a gift offering a clue to what is wrong in the patient’s life, illuminating behaviors and lifestyle habits that produce negative effects for the patient. The patient subsequently works with their health care practitioner to address their entire life from that gift of pain…
Body as machine:
…[Proponents of] alternative medicine … argu[e] that modern medicine views the patient as a machine to be fixed, just as a mechanic may repair a car. They claim that medical treatment relies on technology to treat separate parts of the body that can be detected as broken. Modern medicine, in this straw-man metaphor, attempts to control or quantify every variable, leading to over medicalization and overtreatment… In response to what they view as a brushing aside of the role of mind, emotions, and the entire person in health, alternative medicine argues that the body and spirit must be viewed as a whole, as a part of a wider balance process…
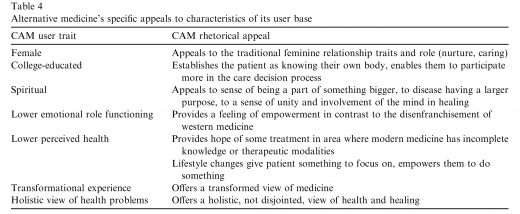
The authors offer a chart that lists the characteristics of typical believers in quackery and how the marketing messages are crafted to appeal specifically to those characteristics:
How can doctors, scientists and public health officials counteract the marketing talents of quacks?
Those who use alternative medicine may be more susceptible to its lure because the rhetoric of these movements appears to be targeted at them. Quackery especially relies heavily on pathos arguments for persuasion while undermining the ethos of modern medicine, appealing to the desire for independent thought process in the spiritually minded, more highly educated demographic. This sets up a moral dichotomy in medicine, where modern medicine is seen as cold, artificial, toxic, and disconnected in comparison to the more personable, natural, pure, and holistic approach of alternative medicine that empowers a patient to be a part of their own healing. Knowing this rhetoric, Western medical practitioners should adjust their interactions with patients to educate, inform, and empower their own patients to be able to make lifestyle changes as well as providing medication therapy.
As I have written in a wide variety of contexts in the past, quackery is a big business promoted by those with extraordinary marketing acumen. Believers in quackery who pride themselves on being resistant to the marketing messages of the business that is medicine should be alerted to the fact that they are easy marks for the unscrupulous marketing messages of the business that quackery, messages that are tailored to appeal to their egos for the purpose of draining their wallets.
