It is perhaps the most powerful claim in the NCB and homebirth advocacy armamentarium. It’s the claim that the US ranks poorly on infant mortality. It’s powerful, it’s shocking and it’s completely false.
I written about this repeatedly over the years. First, infant mortality (death from birth to one year of age) is a measure of pediatric care, not obstetric care. Neonatal mortality (death from birth to 28 days of age) is more accurate, and perinatal mortality (late stillbirths + neonatal deaths) is the most accurate measure of obstetric care. Second, many countries cheat in calculating both infant and neonatal deaths.
How do they cheat? According to the World Health Organization, the infant death rate is the number of infant deaths divided by the total number of live births in a year. Similarly, the WHO definition of neonatal mortality is the number of neonatal deaths divided by the total number of live births in a year. Not surprisingly ALL live born babies, regardless of weight or gestational age are supposed to be included in these calculations. The US adheres to these guidelines, as does Canada. Most other first world countries do not. They cheat by deliberately excluding very premature babies. In other words, they classify the babies who are most likely to die as born dead (and therefore not included) even when they are born alive.
So, for example, a 28 weeker who lives for several days is counted in the US or Canadian neonatal mortality statistics, but is treated in many other countries as if it never existed, thereby artificially lowering the neonatal mortality rate.
This has a huge impact on mortality rates. That’s why other countries cheat in the first place. A paper published last month in the British Medical Journal has quantified exactly how large the impact is. It turns out that the US (and Canada) don’t have poor rankings and never had poor rankings. They actually have among the best ranking for infant and neonatal mortality it the world!
The paper is Influence of definition based versus pragmatic birth registration on international comparisons of perinatal and infant mortality: population based retrospective study, written by multiple scientists at Fetal and Infant Health Study Group of the Canadian Perinatal Surveillance System.
The authors investigated the cheating by determining how many premature babies were included in the mortality rates. They found that most countries besides the US and Canada exclude live born babies less than 500 gm (1 pound, the typical weight at 22-23 weeks gestation and at the outer limit of viability). More surprising, many countries exclude live babies less than 1,000 gm (2 pounds, the typical weight at 28 weeks gestation, and known to have a very high survival rate).
Here is what they found:
Results: The proportion of live births under 500 g varied widely from less than 1 per 10 000 live births in Belgium and Ireland to 10.8 per 10 000 live births in Canada and 16.9 in the United States. Neonatal deaths under 500 g, as a proportion of all neonatal deaths, also ranged from less than 1% in countries such as Luxembourg and Malta to 29.6% in Canada and 31.1% in the United States. Rankings of countries based on crude fetal, neonatal, and infant mortality rates differed substantially from rankings based on rates calculated after exclusion of births with a birth weight of less than 1000 g or a gestational age of less than 28 weeks.
Conclusions: International differences in reported rates of extremely low birthweight and very early gestation births probably reflect variations in registration of births and compromise the validity of international rankings of perinatal and infant mortality.
The following table shows the crude mortality rate for each country (the rate that the country uses) and compares it to the corrected mortality rate. The corrected mortality rate is the neonatal mortality for live born babies of 1,000 gm or more (click on it for a larger view).
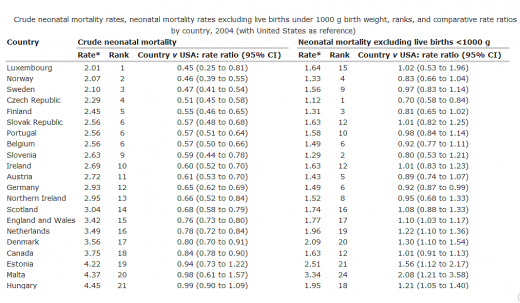
Crude neonatal mortality rates are on the left side of the table. As you can see, the US ranks 22nd, behind countries like Malta and Hungary. However, when the crude results are adjusted by removing all babies under 1000 gm (which weren’t included in the crude rates for most countries), the results are very different. Almost all the countries in the table have a neonatal mortality rate just about the same as the US, or even higher.
The graph below illustrates the results (click on it for a larger view).
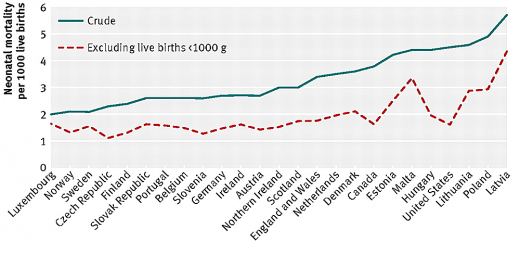
The top line represents crude neonatal mortality rates ranked in rising order. The bottom line represents corrected rates. Now instead of the US having the highest rate of neonatal mortality, it has one of the lowest rates.
How do countries that exclude live born premature infants from mortality rates account for those babies? They categorize them as stillbirths. That’s why perinatal mortality (neonatal mortality + stillbirths) is the most accurate measure of obstetric care. Perinatal mortality does not allow countries to hide premature babies as if they never existed.
The conclusion is clear. International comparisons of crude infant or neonatal mortality rates are invalid. They are grossly inaccurate because many countries cheat in order to make their statistics look better.
The authors note:
The World Health Organization … has long defined a live birth as any product of conception that shows signs of life at birth, with no consideration for birthweight or gestational age criteria. Although this definition remains unchallenged, countries have widely varying regulations for registration of birth that range from definition based to pragmatic. For instance, birth registration is required for all live births that satisfy the WHO’s definition of live birth in Canada, England and Wales, and the United States, whereas countries such as the Czech Republic, France, and the Netherlands specify limits based on some combination of gestational age (for example, at least 22 weeks), birth weight (for example, at least 500 g), or survival (for example, any live birth irrespective of birth weight that survives the first 24 hours after birth). Procedural differences due to longstanding traditions, social attitudes, and local incentives (including financial remuneration of healthcare providers) also probably dictate whether an infant at the borderline of viability is registered…
In summary, we observed large international differences in the reported proportion of live births under 500 g and under 1000 g birth weight and in neonatal deaths in these birthweight categories. International comparisons based on crude fetal, neonatal, and infant mortality rates yielded results that differed from comparisons that excluded extremely low birthweight and early gestation births, especially those at the borderline of viability. Variations in the registration of births at the borderline of viability and related problems compromise the validity of international rankings of industrialised countries by perinatal and infant mortality.
The bottom line is that the US does not now and has not in the past ranked poorly on infant and neonatal mortality. The US has one of the lowest rates in the world and NCB and homebirth advocates should stop lying about it in their efforts to make homebirth look “safe.”