One of the favorite memes of advocates is that natural childbirth is “evidence based,” while obstetricians ignore scientific evidence. Childbirth blog, websites and message boards slap “evidence based” over whatever nonsense they dream up, and figure that the gullible public will look no further.
A good rule of thumb for anyone researching childbirth is this: if a natural childbirth website calls itself “evidence based,” it almost certainly purveying pseudoscience dressed up as science. The website of cardiology nurse Rebecca Dekker, Evidence Based Birth is a prime example. As the saying goes, you can put lipstick on a pig, but it’s still a pig, and in the world of childbirth, “Evidence Based Birth” is a big fat pig covered with lots of lipstick.*
How can you tell the difference between science and pseudoscience dressed up as science? This image from I fucking love science lays out the general principles.
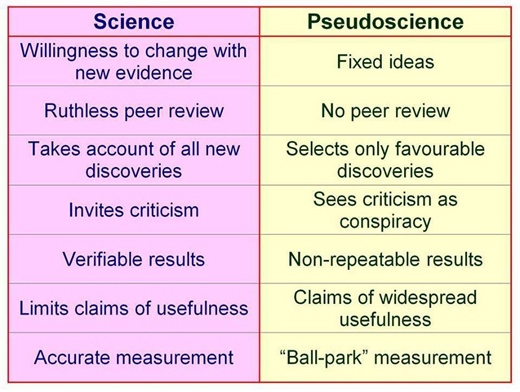
The primary difference between science and pseudoscience is a willingness to change based on new evidence. Pseudoscience, in contrast, starts with a conclusion and defends it regardless of the evidence.
Rebecca Dekker starts with the premise that the tenets of natural childbirth are true and looks for evidence that confirms those tenets. She ignores evidence that does not support natural childbirth, and is not above deliberately misleading readers by posing one question, but answering another.
Her recent piece on waterbirth, Evidence on the Safety of Water Birth, is a classic in this genre. Dekker starts with the premise that waterbirth is safe and cherry picks evidence to support that claim while ignoring or inappropriately dismissing evidence that shows the opposite.
What is waterbirth? It is the practice of giving birth a plastic pool of water that is inevitably fecally contaminated. It is the equivalent of giving birth in a toilet, and has similar risks, including the risk that the baby will breathe in or swallow the fecally contaminated water.
The American Academy of Pediatrics’ Committee on Fetus and Newborn in conjunction with the American College of Obstetricians and Gynecologists has recently updated its position on waterbirth. Nothing has changed since the previous edition published in 2005, except in the intervening years more cases of perinatal death and injury have been reported.
Some of the reported concerns include higher risk of maternal and neonatal infections, particularly with ruptured membranes; difficulties in neonatal thermoregulation; umbilical cord avulsion and umbilical cord rupture while the newborn infant is lifted or maneuvered through and from the underwater pool at delivery, which leads to serious hemorrhage and shock; respiratory distress and hyponatremia that results from tub-water aspiration (drowning or near drowning); and seizures and perinatal asphyxia. (my emphasis)
But, hey, that’s just the way that the American Academy of Pediatrics’ Committee on Fetus and Newborn and the American College of Obstetricians and Gynecologists assess the scientific literature. Cardiology nurse Rebecca Dekker thinks she knows better.
Her piece contains lots and lots and lots of words, but her conclusion is pretty simple. The evidence that currently exists is less than the highest quality evidence.
Duh!
The AAP and ACOG are well aware of that. They are invoking the precautionary principle. What’s the precautionary principle?
According to Wikipedia:
The precautionary principle … states that if an action or policy has a suspected risk of causing harm to the public or to the environment, in the absence of scientific consensus that the action or policy is not harmful, the burden of proof that it is not harmful falls on those taking an action.
In other words, in the absence of high quality evidence that waterbirth is safe, it should not be standard care. AND it is up to the proponents of waterbirth to provide that high quality evidence before waterbirth can be recommended.
But Dekker completely ignores the precautionary principle in her conclusion.
According to Dekker:
Based on the data that we have, waterbirth is a reasonable option for low-risk women during childbirth, provided that they understand the potential benefits and risks. If women have a strong desire for waterbirth, and there are experienced care providers who are comfortable in attending waterbirths, then at this time there is no evidence to deny women this option of pain relief.
Simply put, the AAP and ACOG believes (in conjunction with Dekker) that there is no high quality evidence to support waterbirth, and a growing body of lower quality evidence that waterbirth kills babies who breathe in the fecally contaminated water or swallow it during birth. Dekker starts with the conclusion that waterbirth must be safe, dismisses the existing evidence on the deaths that resulted from waterbirth, and asserts that it must be considered safe until it is definitely proven to be deadly. Dekker’s claim about the safety of waterbirth isn’t evidence based; it’s her opinion.
The same thing goes for nearly everything on her site. That is presumably why Dekker isn’t spending any time speaking in any venue where she could educate pediatricians or obstetricians about their purported errors in evidence interpretation. She knows she’d be laughed off the stage. She isn’t writing for physicians or scientists, either, because they would eviscerate her claims in short order. She writes for lay people who aren’t capable of assessing the validity of her claims and, in many cases are merely looking for justification to ignore the advice of pediatricians and obstetricians.
A more accurate moniker for her website would be “Rebecca Dekker’s Opinion on Birth,” but who is going to take that seriously? Instead, she calls it “Evidence Based Birth.” Dekker can put lipstick on a pig of a website, but it’s still a pig.
*Dekker basically admits this in her website disclaimer:
The information presented here does not substitute for a healthcare provider-patient relationship nor does it constitute medical advice of any kind… The opinions expressed in this blog are strictly the author’s personal opinions … The information on this blog may be changed without notice and is not guaranteed to be complete, correct, timely, current, or up-to-date…(my emphasis)