
The new out of hospital birth study, Planned Out-of-Hospital Birth and Birth Outcomes, by Snowden et al. is getting a lot of media attention.
As I explained in yesterday’s post the authors deliberately soft pedaled the findings:
Dr. Aaron Caughey, a co-author who heads the university’s obstetrics department, said the researchers consciously adopted a nonjudgmental tone so critics would not say that the in-hospital providers were demonizing out-of-hospital births.
That strategy seemed to have worked to mute the criticism of homebirth supporters, but the fact is that the increased risk of death at out of hospital birth isn’t small all. To understand why, it helps to compare the death rates at out of hospital birth to the death rates from SIDS.
[pullquote align=”right” color=”#000000″]The absolute increased death rate from out of hospital birth far exceeds the absolute increased death rate of placing a baby to sleep on her stomach.[/pullquote]
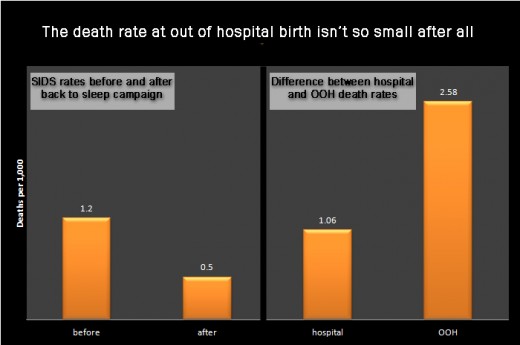
SIDS haunts the nightmares of new parents and prospective parents. It is so frightening because apparently healthy infants die suddenly for no discernible reason. The first real breakthrough in preventing infant deaths from SIDS came with the “back to sleep” campaign when researchers noted that babies were more likely to die of SIDS when sleeping in their stomachs than on their backs. Since the beginning of the campaign, death rates from SIDS have dropped from 1.2/1000 in 1992 to 0.5/1000 in 2010. The campaign is considered a great success and it is the rare parent who ignores the advice.
Who would now say that the increased risk of death from infants sleeping on their stomachs is acceptable because the absolute risk of death is small? No one, right?
So how can it be that the increased risk of death at out of hospital birth from 1.06/1000 to 2.58/1000 is acceptable because the absolute risk of death is small?
Here’s a bar chart that sets out the absolute rates of death. You can see that the absolute increased death rate from out of hospital birth far exceeds the absolute increased death rate of placing a baby to sleep on her stomach.
Out of hospital births ought to haunt the nightmares of prospective parents. It should be frightening when apparently healthy infants die for entirely preventable reasons especially when the increased risk of death is far larger than the increased risk of death from SIDS when ignoring the back to sleep warning.
Drs. Snowden, Caughey and their colleagues are to be congratulated for publishing a paper that is so clear, meticulous and measured that even the homebirth community cannot argue with that finding that out of hospital birth more than doubles the risk of perinatal death. As Dr. Caughey noted, the authors chose a non-judgmental tone so that homebirth advocates would not be able to accuse them demonizing out of hospital birth.
But the increased risk of death at out of hospital birth isn’t small after all. The mainstream media and American women should take note.
You can find the SIDS statistics here.