Natural childbirth advocates are in danger of losing their minds.
Obstetricians have been discussing the data that shows that routine induction at 39 weeks may be safer than waiting for labor to begin on its own. The possibility of consensus on this issue was discussed at the recent annual meeting of the American College of Obstetricians and Gynecologists. As the Washington Post explained:
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Nature is a terrible midwife.[/pullquote]
Norwitz argued against simply letting nature take its course.
“Nature is a terrible obstetrician,” he said, referring to the “continuum” of pregnancy and birth: the large number of zygotes that never implant, the 75 percent lost before 20 weeks, and stillbirth.
And, he said, the risk of stillbirth and neurological injuries rises after 39 weeks. “Stillbirth is a hugely underappreciated problem,” he said. “There are anywhere between 25,000 to 30,000 stillbirths a year in the United States.”
Indeed, the argument can be summarized in a simple graph:
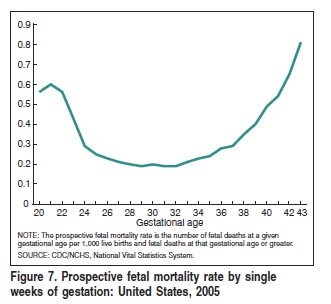
This is a graph of stillbirths vs. gestational age. As you can see, the stillbirth rate begins to rise precipitously at 36 weeks. But babies born at 36 weeks have a small but significant risk of immature lungs leading to breathing problems requiring intensive care. The graph below summarized the data of 3 studies on the risk of lung immaturity.
The lines on the two graphs cross at approximately 39 weeks when the risk of lung immaturity is 0% and the stillbirth rate continues to rise.
In other words, the optimal time for birth is at 39 weeks gestation.
Not surprisingly, natural childbirth advocates are horrified.
Cristen Pascucci, an advocate for giving women more control over childbirth decisions, thinks the doctors’ remarks suggest that all babies need to be “rescued by birth,” creating an anti-woman mentality. “It’s as if women and their babies are fundamentally in opposition to each other and the female body is dangerous by design,” said Pascucci, a vice president of the advocacy group Improving Birth.
It calls into question the fundamental conceit of the natural childbirth movement that childbirth is inherently perfect. But nature is a terrible midwife; the day of birth is the single most dangerous day in the 18 years of childhood. The risk of a baby dying on the day of birth is not exceeded until that baby is 92 years old.
Childbirth, like any aspect of body function, is subject to the multiple competing demands of natural selection.
Natural childbirth advocates don’t seem to understand that natural selection leads to the survival of the FITTEST, not survival of everyone. Those that aren’t fit often simply die.
For example, the distinguishing feature of human beings is their large brains. Overall, large brains confer a tremendous evolutionary advantage at birth and throughout life. The larger the brain at birth, the more neurologically mature the newborn and the better the chances of its survival.
But large brains are an evolutionary disadvantage. That’s because the size of the maternal pelvis has an upper limit. As the maternal pelvis gets bigger, the mother’s ability to walk and run decreases.
Every single birth involves an evolutionary compromise between the neurological advantages of a larger neonatal brain and the potentially deadly consequences of a larger neonatal brain leading to obstructed labor. Prior to the advent of modern obstetrics, babies whose heads were too big to fit simply died and their mothers died with them.
The brain continues to grow throughout pregnancy. Babies born at later gestational ages have bigger heads and are more neurologically mature but also more likely to die in labor. Babies born at earlier gestational ages have small heads which gives them a tremendous advantage in childbirth.
The same thing applies to the size of babies relative to the function of the placenta. Some placentas last longer than others. The longer a baby remains inside the mother, the more neurologically mature and fitter it will be. However the longer a baby remains inside the mother, the greater the chance that its growth will outstrip the placenta’s ability to supply oxygen. If the baby stays inside longer than the placenta can function, the baby is stillborn. The timing of birth represents a compromise between these competing imperatives.
Natural childbirth advocates are fond of pointing out that the a due date is just an estimate; a baby can be born any time between 38 weeks and 42 weeks or beyond. But they draw the wrong conclusion from this. They ascribe the variation in length of pregnancy to necessity (“a baby knows when to be born”) when it is merely due to evolutionary chance.
The idea that a baby knows when to be born and therefore is always born at the perfect time makes as much sense as the idea that a nose “knows” how big to grow and therefore everyone’s nose is the perfect size for her face. It makes as much sense as claiming that everyone’s blood pressure “knows” the ideal level to prevent heart attack or stroke, or that everyone grows to a perfect height. In other words, it makes no sense at all.
If babies truly knew when to be born, the first graph above would be a straight line; there would be the same number of stillbirths at every gestational age. That clearly is not the case. Babies DON’T know what to be born.
No wonder natural childbirth advocates are spluttering.
But their spluttering also illustrates another fundamental problem with natural childbirth. It’s not a matter of science, but of belief.
The Washington Post article reports that the ACOG debate changed the minds of many obstetricians in the audience. When presented with new scientific information, they reached new conclusions. In contrast, natural childbirth advocates would not give up cherished beliefs (“natural is better”), regardless of the evidence they were shown.
It reminds me of the debate on evolution between Bill Nye and creationist Ken Hamm. When Nye was asked was asked what would convince him that creationism was true, he responded, “Evidence.” When Hamm was asked what would convince him that evolution was true, he answered in effect, “Nothing.”
Natural childbirth advocates are like Ken Hamm. They start with the conclusion and work backward trying to cherry pick evidence to support it. They’re spluttering because no amount of evidence will ever change their minds.