
I, I, me, me, my birth, my VBAC, my experience, just me, always me!
On Wednesday, I wrote about Dr. Brad Bootstaylor and See Baby Midwifery. DeKalb Medical Center restricted Dr. Bootstaylor’s privileges allegedly in the wake of a profoundly injured baby resulting from an attempted homebirth after two previous C-sections.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]What about the babies who have been harmed? Who gives a shit?[/pullquote]
Apparently that was one injured baby too far, and DeKalb moved to protect mothers and infants (and itself) from a doctor who allegedly violated evidence based standards of care in obstetrics and demonstrated lack of clinical judgment and skill; even his supporters acknowledge that “forceps are not his strong suit.”
How dare the hospital try to protect babies and mothers from allegedly incompetent and dangerous providers? Who gives a shit about injured babies and heartbroken mothers? Certainly not the narcissists in the protest group organized to oppose the dastardly requirement for clinical competence.
They got a lawyer, the husband of one of See Baby’s pregnant clients, Zawn Villines, and began threatening the hospital.
She explains:
By Sunday, we were prepared to begin writing letters. Jeff [Filipovits] sent his first lawyerly letter to the hospital, and many group members began doing the same. This letter-writing campaign continued, and group members began sharing their letters. Jeff had numerous communications with the hospital, was threatening a lawsuit, and knew the specific causes of action under which he could file one.
Then, like a bad penny, Dawn Thompson from ImprovingBirth.org turns up counseling more intimidation:
Dawn Thompson of ImprovingBirth. org got in on things to offer us behind-the-scenes help. She suggested the second protest on Labor Day that we began using as a threat. Many other birth advocates and professionals also got involved early to lend resources. They include, but are not limited, to Brenda Sanders Parrish, Debbie Pulley, Kim Baxley Wilson, and so many more.
Then they met with the hospital to threaten them with a barrage of lawsuits:
Wednesday, we met with the hospital. Jeff made various legal threats. We all made threats. It was not at all a friendly meeting. In fact, I would say that members of our group were more hostile, more aggressive, and more demanding than I have ever seen anyone be in any other negotiation. They were also smart. We didn’t go in and yell. We went in prepared to ask legal questions, to accuse their lawyer of practicing medicine without a license, to threaten lawsuits over forced episiotomies, and so much more.
What about the profoundly injured HBA2C baby and other babies who have been harmed? Who gives a shit? Certainly not the “birth warriors” threatening the hospital.
They were planning their next protest when the hospital’s lawyer called, offering:
*Reinstatement of Dr. B’s VBAC and vaginal breech delivery privileges (except for VBAC3)
*Agreement to provide us with full details about the water birth vote on Monday, as well as agreement that we will get full details about future actions well before October 31.
*Reinstatement of vaginal breech delivery (Dr. B is still the only physician currently providing it)…
*Relaxation of IV and eating rules–please note they’re still saying it’s “hospital policy,” so you will need to be prepare to give a firm no.
What about the babies who have been harmed? Who gives a shit?
There was some sort of quid pro quo:
We canceled the protest for legal reasons we cannot disclose here. This is not an attempt at secrecy, but a recognition of the challenging realities of threatened litigation and hospital politics.
Please understand that if we still had the protest, it is very likely we would lose every single gain we made. That affects real laboring women right now. Their lives are different and better because of this movement. No one’s life has been made worse because of this movement.
What’s next for these intrepid birth warriors?
*Targeted protests against problematic birth policies; we could be like a birth strike force.
*Targeted lawsuits against birth policies, forced interventions, and medical malpractice.
*Working to end the water birth and VBA3C ban …
And, of course:
A new, moderated group that requires a signed commitment to confidentiality to avoid being infiltrated by the Skeptical OB and others (please note anything you say here is effectively public, since the media is here, as well as people who wish to make this group look foolish).
Hey, that’s not right! I’m not trying to make you look foolish. I’m trying to make you look like people who don’t give a shit about dead or injured babies, and you’re helping me do it.
No one has suggested that the hospital is acting for any reason other than to protect babies and mothers. Zawn Villines, Dawn Thompson et al. are threatening to sue the hospital to force them to STOP protecting babies and mothers.
It may be legal, but it is both ugly and unethical.
Update: See Baby Midwifery supporters are attempting to pitch NPR a story that DeKalb Medical Center is threatening women with with physical force.
Here’s how they intend to make the case:
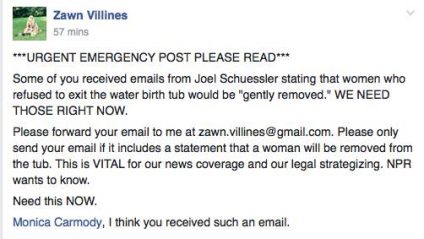
***URGENT EMERGENCY POST PLEASE READ***
Some of you received emails for Joel Schuessler stating that women who refuse to exist the water birth tub would be “gently removed.” WE NEED THOSE RIGHT NOW.
…This is VITAL for our news coverage and our legal strategizing. NPR wants to know.
I need this NOW.

L: … Here’s what mine said: “In the event that waterbirths are discontinued permanently, policies and procedures will be in place to safely removed mothers who wish to labor in water to another setting for delivery.”
Zawn: you may have just won this for us
But ACOG and the AAP have clinical guidelines that say waterbirth is dangerous for babies.
Who gives a shit about the babies?
Where does Dr. Bootstaylor stand on what has been happening?

“THANK YOU” everyone from my inner core to outer sanctum in the spirit of honoring birth, choices, and shared decision making.
I’m truly humbled and honored to be in alignment with all Mothers and Families
Bring Birth Back!
What about the babies that have been harmed or will be harmed?
All together now: Who gives a shit about the babies?