
More babies die of infection at homebirth than at hospital birth.
Surprised?
Homebirth advocates often insist that homebirth is beneficial because it avoids exposing babies to infections. That claim always made little sense on its face since the major infectious causes of neonatal death, group B streptococcus and herpes, are found in the mother’s vagina. Now a new paper by Grunebaum et al. confirms that the high death rate at American homebirth includes an increased risk of death from infections that would have been easily prevented or treated at the hospital.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Homebirth increases the risk of neonatal death from infection.[/pullquote]
The paper is Underlying causes of neonatal deaths in term singleton pregnancies: home births versus hospital births in the United States.
The authors note:
Midwife-attended home births in the United States (US) are associated with an increase in adverse neonatal out-comes such as a higher incidence of neonatal mortality (NNM), Apgar score of 0 at 5 min, and neonatal seizures or serious neurologic dysfunction, but the causes for the increase in NNM in home birth have not been reported previously. The objective of this study was to evaluate the underlying causes of NNM in midwife-attended home births and compare them to hospital births attended by a midwife or a physician in the US.
What did they find?
Overall, the midwife-attended home births had the highest rate of neonatal deaths (122/95,657 NNM 12.75/10,000; RR: 3.6 (95% CI 3–4.4), followed by hospital physician births (8,695/14,447,355 NNM 6.02/10,000; RR: 1.7 95% CI 1.6–1.9) and hospital midwife births (480/1,363,199 NNM 3.52/10,000 RR: 1)…
Among midwife-assisted home births, underlying causes attributed to labor and delivery caused 39.3% (48/122) of neonatal deaths (RR: 13.4; 95% CI 9–19.9) followed by 29.5% due to congenital anomalies (RR: 2.5; 95% CI 1.8–3.6), and 12.3% due to infections (RR: 4.5; 95% CI 2.5–8.1).
By and large, labor and delivery issues refer to oxygen deprivation from a variety of different sources: inability to perform a timely C-section through inability to perform an expert neonatal resuscitation. It’s only to be expected that most of the deaths at homebirth are attributed to not being at a hospital.
Congenital anomalies as a cause of death is also an expected finding since that is the major cause of death for term babies in hospitals.
But the fact that infection is the 3rd leading cause of death at homebirth thoroughly debunks the claim of many homebirth advocates that a key benefit of homebirth is avoiding infections. You don’t avoid neonatal infections by giving birth at home because the infectious agents are in the mother’s vagina, not the hospital environment. The difference in infectious deaths at home vs. the hospital is because hospitals prevent infections by prophylactic antibiotics for group B strep and elective C-sections for active herpes.
The results are represented by this graph:
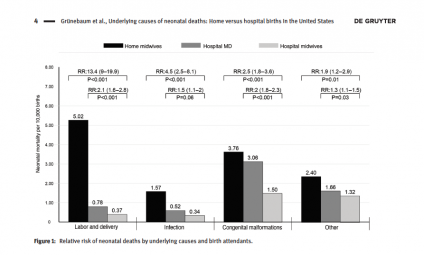
The authors conclude:
Our study shows that the significantly increased risks of neonatal deaths among midwife-attended home births are associated with three underlying causes: labor and delivery issues, infections, and fetal malformations. Each of these underlying causes was significantly increased when compared to midwife-attended hospital births.
The hospital NNM in our study is similar to the NNM reported for 2010 in the US by Matthews and Mac-
Dorman. This study’s significantly elevated term NNM of 12.75/10,000 births for home births confirms
the increased neonatal mortality risks reported among midwife-attended home births by other US home birth studies: Cheyney et al. reported a NNM of 12.3/10,000 from 2004 to 2009 and Grunebaum et al. reported a term NNM for home births of 12.6/10,000 from 2006 to 2009.
They note that homebirth is much more dangerous in the US than in other industrialized countries:
Other studies on homebirth outcomes such as studies from the Netherlands, Ontario and British Columbia, where homebirths are well integrated in the health system, found no increased risk of adverse perinatal outcomes for planned home births among low-risk women …
American homebirth midwives (CPMs and LMs) lack the education and training of all other midwives in the industrialized world including US certified nurse midwives (CNMs) and midwives in the Netherlands, the UK, Canada, Australia, etc.
American homebirth kills babies. Avoiding the hospital doesn’t merely increase the risk of a baby dying from oxygen deprivation; it also increases the risk of a baby dying of infection.