Natural childbirth advocates employ birth affirmations as a form of magical thinking. They appear to believe that if they just wish hard enough, they can affect the likelihood of the unmedicated vaginal birth that they are supposed to want.
That’s nonsense, of course. But birth affirmations are also anti-feminist. They are anti-feminist because they assume that a woman’s virtue resides in her vagina, because they ignore women’s needs and desires, and because they arise from philosophies that seek to immure women back into the home.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]A woman’s virtue does not reside in her vagina.[/pullquote]
My feminist mothering affirmations rest on the opposite premises:
- A woman’s virtue resides in her mind, talents and character. Whether or not a baby transits her vagina is no more important than whether or not she wears glasses.
- Women’s needs — for pain relief in labor, for control of whether their breasts are used to feed their babies, for participation in the world beyond mothering — are more important than any purported benefits from natural childbirth, breastfeeding or attachment parenting. Whether or not a woman chooses to adhere to these philosophies is her decision, based on what she thinks is best for her children, not what other people, ignoring scientific evidence, think is best for her children.
- Women — and society — benefit when they are encouraged to use the full range of their talents in the wider world, and women — and society — are harmed when women are immured in the home, forced to restrict themselves to childcare.
Here are my top ten feminist mothering affirmations:
1. It makes no difference how my baby is born.
Over the course of your son or daughter’s childhood, you will have many occasions to ponder how your actions impact your child’s life and you will second guess yourself many times, wondering if you had handled a specific situation differently might your child have been happier or more successful. Whether your baby was born vaginally or by C-section should never be one of them. It will make absolutely, no difference to your child how he or she emerged from your womb (or, in the case of an adopted child, even if he or she emerged from your womb). There is no reason for you to worry or obsess about how your baby is born.
2. There is no reason for me to suffer.
Some lucky women have a manageable amount of pain in labor and don’t need any relief. Most, however, have an unmanageable amount of pain and desperately seek relief. There is NO REASON to forgo pain relief when you are in pain. It is not safer, healthier or better in any way for your baby or for you to withstand hours of excruciating pain.
3. I am not in competition with other women.
Admittedly this is hard to believe when your friends, acquaintances and casual strangers demand details of your birth so they can compare their “performance” to your “performance,” but it’s true. It’s nobody’s business how you choose to give birth to your child and they don’t deserve to comment upon or even to know those private details.
Childbirth is not a performance that ought to be rated or compared. Childbirth is a bodily function like vision. Sometimes it works well; sometimes it needs help. No one judges women who wear glasses or contacts for nearsightedness even though their eyes don’t work “as nature intended.” Nearsightedness just happens, is no one’s fault and implies nothing about the overall health or quality of a woman’s body. Similarly, childbirth complications just happen, are no one’s fault and imply nothing about the overall health or quality of a woman’s body.
4. I am not guaranteed a healthy baby, so I need to consult with the professionals who can help me ensure my baby’s health.
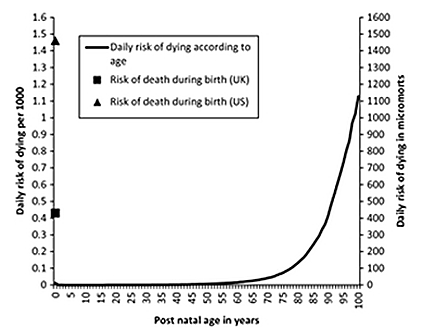
Human reproduction, like all reproduction, has a high degree of “wastage,” which is another way of saying that death is a common complication of pregnancy. For example, 1 in 5 established pregnancies will end in miscarriage. No amount of wishing and hoping will change that. Similarly, in nature, nearly 10% of pregnancies will end in the death of the baby, the mother or both. Fortunately, the interventions of modern obstetrics can prevent the vast majority of those deaths, but only if you avail yourself of those interventions and the expertise of the people trained to use them.
5. I will not trust birth, because birth is not trustworthy.
Trusting birth makes about as much sense as trusting vision. No amount of trusting will prevent nearsightedness, so refusing eye exams in favor of trusting vision is stupid in the extreme. That goes double for childbirth, which is far more deadly than nearsightedness.
6. I will carefully analyze the motives of those who declare that any particular way of giving birth is “better” than any other.
When you take the time to analyze the advice and recommendations of “birth workers” like midwives, doulas and childbirth educators, ask yourself if they profit when you follow their advice. That does not mean that their advice is necessarily wrong, but it can and too often does compromise their recommendations. Instead of recommending what is good for you and your baby, they may be recommending what is good for their wallet.
Similarly, you should analyze the advice and recommendations of friends and acquaintance looking at how they benefit if you do what they suggest. Are they anxious for you to validate their birth choices by making the same choices? If so, feel free to ignore them.
7. I will not take pregnancy advice or care from anyone who won’t take responsibility for that advice or care.
If a homebirth midwife doesn’t carry insurance, and makes you sign a document declaring that the responsibility for any and all outcomes in yours, she is signaling that even she doesn’t believe that she is educated enough or trained enough to take responsibility your baby’s life or for your life. Real professionals take legal and ethical responsibility for their work; amateurs and hobbyists never do.
8.My baby does not care whether he or she is breastfed or bottlefed.
It makes literally no difference to the baby how he or she gets fed, only that he or she gets fed. Yes, breastfeeding does have some advantages, but those advantages are small and in industrialized countries those benefits are trivial.
9. Both the baby’s needs and my needs matter when it comes to infant feeding.
Yes, breastfeeding can be difficult and stressful in the first few days and weeks, and it is great to persevere through those difficulties if breastfeeding is important to you. But the baby’s hunger and suffering count for a lot, and if you feel your baby is suffering from hunger, you should feel free to feed the baby formula. Your pain and suffering count, too. If your nipples are raw and bleeding, if you have horrible pain when nursing, if you start crying every time the baby cries with hunger, dreading nursing, it is perfectly healthy and acceptable to use formula instead, either for supplementing or exclusively.
10. I will not judge my mothering by the performance of my body.
You mother with your entire body. Your arms hold and embrace your children. Your hands guide. Your lips kiss. Your brain plans and worries, and your metaphorical heart loves your child. Your uterus, vagina and breasts are trivial when compared to the other body parts, so it makes no sense to judge your mothering by whether you had a vaginal birth or breastfed your children.
Mothering is hard. I know; I have four children and I have spent countless hours caring and worrying, wishing I could carry their burdens, smooth their paths, and absorb their hurts. My children are adults now, and no doubt there are many things that they think I could have done better, but they never, ever give any thought to their route of delivery or to whether or for how long they are breastfed.
Don’t judge yourself on these issues, and don’t let anyone judge you. It isn’t simply doesn’t matter and it’s anti-feminist.
Adapted from a piece that first appeared in August 2014.