Ahhh, the power of the press release.
Evidently the folks in the PR office of the “journal” Birth: Issues in Perinatal Care have been working overtime. They’ve sent out thousands of press releases touting the latest study by MacDorman and colleagues purporting to show the the rate of homebirth in the US has risen 20% (from a teeny, tiny number to a bigger teeny, tiny number) during the years 2004-2008.
The public relations campaign that is promoting the paper implies that there has been a meaningful and substantial increase in the rate of planned homebirths in the US as a direct result of women rejecting hospitals and hospital based interventions. Is that what the paper shows? Not exactly, not least because it doesn’t even bother to distinguish between planned and unplanned homebirths.
Marian MacDorman et al., authors of the paper, United States Home Births Increase 20 Percent from 2004 to 2008, claim:
In 2008, there were 28,357 home births in the United States. From 2004 to 2008, the percentage of births occurring at home increased by 20 percent from 0.56 percent to 0.67 percent of United States births. This rise was largely driven by a 28 percent increase in the percentage of home births for non-Hispanic white women, for whom more than 1 percent of births occur at home. At the same time, the risk profile for home births has been lowered, with substantial drops in the percentage of home births of infants who are born preterm or at low birthweight, and declines in the percentage of home births that occur to teen and unmarried mothers. Twenty-seven states had statistically significant increases in the percentage of home births from 2004 to 2008; only four states had declines.
But even a brief glimpse at the methods used by the authors to calculate the rate of homebirths reveals that numbers quoted are nothing more than “guesstimates” based on proxies for real data.
In order to accurately determine the number of planned homebirths in the US, we’d need to know the number of women who planned to have a homebirth and successfully did so, the number of women who planned to have a homebirth and ultimately delivered in the hospital, as well as the numbers of babies who were born dead during homebirth. That’s not what the authors looked at.
MacDorman and colleagues looked at birth certificates to determine whether a birth occurred inside or outside of a hospital. In fact, the authors used the exact same technique used in part of the Wax study, a technique bitterly criticized by homebirth advocates specifically because it failed to distinguish between planned and unplanned homebirths.
So what did the authors actually find? They discovered that in 2004 there were 23,150 births that took place outside the hospital and in 2008 there were 28,357 births. Then the authors made a leap of faith, or rather several leaps of faith. MacDorman et al. ASSUMED the ratio between planned and unplanned homebirths remained the same from 2004 to 2008. They ASSUMED that the rate of hospital transfer during planned homebirth remained the same from 2004 to 2008. They ASSUMED that the death rates of planned homebirth remained the same from 2004 to 2008.
Those are big assumptions to make about a dataset composed of very small numbers (relative the to overall number of births). It is entirely possible that some portion of the purported “increase” that they observed reflected NOT an increase in the number of planned homebirths, but an increase in the number of unplanned homebirths. It is equally possible that some portion of the purported “increase” that they observed reflected NOT an increase in the number of planned homebirths, but a decrease in the number of hospital transfers. It is equally possible that some portion of the purported “increase” that they observed reflected NOT an increase in the number of planned homebirths, but a decrease in the number of homebirth deaths. And, of course, it is very possible that a substantial proportion of the purported “increase” in planned homebirths actually reflects some combination of the three.
The authors are anything but subtle in their motivation for publishing this study. They announce their motivation in the abstract:
Conclusion: The 20 percent increase in United States home births from 2004 to 2008 is a notable development that will be of interest to practitioners and policymakers.
In other words, this is an attempt to convince policy makers that the rate of planned homebirth is rising and that, therefore, there is a demand for more homebirth practitioners.
If that wasn’t clear enough, the “journal” Birth released the article on-line four months before actual publication. How ironic is that? Homebirth advocates, the very same people who bitterly criticized the early on-line publication of the Wax study and denounced it as an attempt to influence public policy respond by attempting to influence public policy with an article published online even farther in advance.
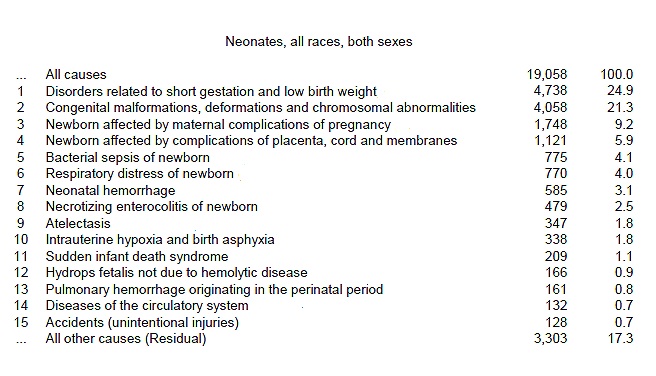
Of course, the MacDorman paper fails utterly to address the most serious concern about homebirth, the increased risk of perinatal death. The authors enthusiastically boast that the rate of “homebirth” has risen without bothering to find out how many babies died in the process.
That’s fairly typical in the world of homebirth advocacy. And increase in homebirth rates is a cause for celebration. Who cares how many babies died as a result?