When I was a third year medical student, a surgery resident on my team hit on me.
It was exceedingly unpleasant and rather surprising since I made it clear that I was happily married. That didn’t deter him from making a suggestive phone call at 2 AM waking me from sleep in the on call room adjacent to his.
The next morning I reported his behavior to the Director of Surgery who immediately declared: “That didn’t happen!”
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Imagine if the scientific literature were filled with papers referring to sexual harassment as “perceived sexual harassment”.[/pullquote]
When I insisted that yes, indeed, it had happened, he announced that he was sending me to a psychiatrist to find out what was wrong with me; henceforward I would be viewed as a trouble maker.
The Director was engaged in a form of epistemic injustice known as testimonial silencing.
Every day breastfeeding professionals do the same thing to women who experience breastfeeding complications.
According to the Wikipedia article about epistemic injustice:
The term was coined by Miranda Fricker in 2007 …
In Fricker’s 2007 book Epistemic injustice: power and the ethics of knowing, she defines two kinds of epistemic injustice: testimonial injustice and hermeneutical injustice… [T]estimonial injustice occurs when someone’s knowledge is ignored or not believed because that person is the member of a particular social group … A hermeneutical injustice occurs when someone’s experience is not understood (by them or by others) because there are no concepts available that can adequately identify or explain that experience.
My report of sexual harassment was not believed because I was a woman. I was immediately pathologized as a liar and labeled a troublemaker.
Breastfeeding professionals routinely treat women with breastfeeding complications exactly the same way. They aren’t believed; they are pathologized and they are viewed as trouble makers.
Tactics of testimonial silencing include: erasure from breastfeeding literature, refusal to believe, pathologizing, claiming “lack of support,” disparaging women’s stories and banning from social media feeds.
1. Breastfeeding professionals erase women who experience physiological complications from the breastfeeding cannon.
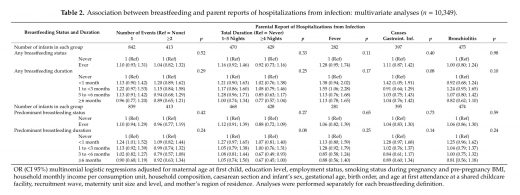
Although breastfeeding complications are common — insufficient breastmilk alone is experienced by up to 15% of women in the days after birth — the breastfeeding literature routinely ignores reality in favor of fantasy, claiming falsely that breastfeeding complications are rare.
It’s the equivalent of insisting that sexual harassment in the workplace is rare. If you’ve been taught that sexual harassment uncommon, you are unlikely to look for it, recognize it or know how to deal with it. Your first response may be: “That didn’t happen.”
The same thing applies to breastfeeding professionals and complications. When you are taught they are rare, you are unlikely to look for them, recognize them or know how to deal with them when they occur. The first response when faced with breastfeeding complications is often: “That’s not what’s happening.”
It would be difficult to overemphasize the impact of the erasure of breastfeeding complications from the breastfeeding literature. It serves as the proximate cause as well as the justification for the testimonial silencing that follows.
2. Women aren’t believed.
Imagine if the scientific literature were filled with papers referring to sexual harassment as “perceived sexual harassment”. The implication would be that women who report sexual harassment at work cannot be believed; they must have “misperceived” the interaction. Only others can judge what “really” happened because a woman’s judgment is not reliable.
The breastfeeding literature is filled with papers referring to insufficient breastmilk as “perceived insufficient milk.” The implication is that women who report insufficient breastmilk cannot be believed; they must be “misperceiving” their babies cries of hunger. Since women’s judgment can be dismissed out of hand as unreliable, only breastfeeding professionals can judge what “really” happened.
3. Women are pathologized.
The first response of breastfeeding professionals to women who report complications is to pathologize the reporters. At best, reporters are pathologized as incorrect in their assessment and not trying hard enough to make breastfeeding work. At worst, they are pathologized as lazy, selfish women who are looking for an excuse not to breastfeed.
Since breastfeeding complications are supposedly so rare as to have been nearly erased from the professional literature, those who report them must have sinister motivations in making claims that can’t be true.
4. “Head patting”
There are many ways to ignore and undermine women’s claims while pretending to take them seriously. In the case of breastfeeding complications, head patting takes the form of claiming “lack of support.” Breastfeeding complications are routinely dismissed by insisting that women just need more breastfeeding support.
Tell lactation professionals that breastfeeding is painful and they’ll insist that it wouldn’t be painful if you had received support.
Tell lactation professionals that your nipples are cracked and bleeding and they’ll claim that wouldn’t have happened if you had received more support.
Tell lactation professionals that you don’t produce enough breastmilk and they’ll tell you that you would be producing enough if only you had the correct support.
5. Disparaging women’s stories of complications.
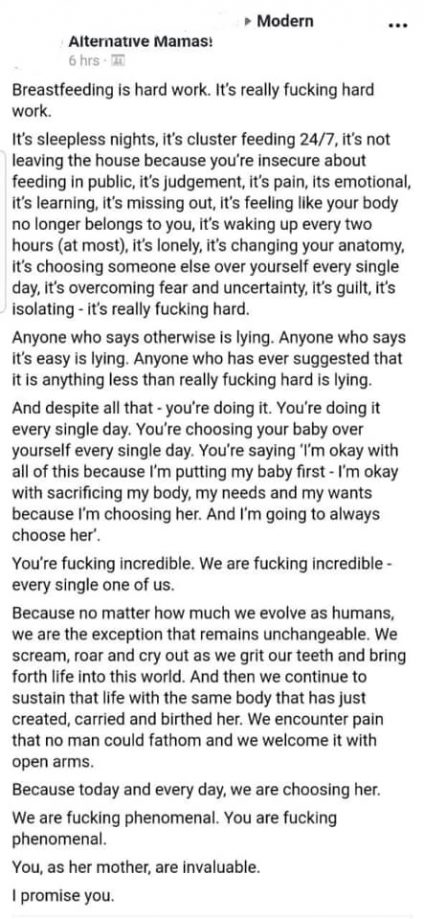
You can’t make this tactic any clearer than Prof. Amy Brown did in her horrible piece Here’s Why You Should Ignore Those Breastfeeding Horror Stories:
Try not to pay too much attention to breastfeeding horror stories. People like to share stories – it makes them feel better – without thinking about the consequences for you.
Women claim they experienced breastfeeding complications? Just ignore them!
6 Banning from social media feeds.
Amy Brown is a master of another tactic of testimonial silencing, banning those who report breastfeeding complications from her social media feeds. She is hardly alone in making her social media “complication free.” No doubt she and her colleagues would justify it as deleting and banning trolls. But what does it say about them that they view women who have suffered and whose babies have suffered as nothing more than trolls? It’s no different from labeling women who report sexual harassment as trolls.
Social media banning completes the practice of testimonial silencing begun by the erasure of women with breastfeeding complications from the scientific literature.
Women are no longer willing to go along with the testimonial silencing of sexual harassment. In my case, the dean of my medical school believed me, although he told me that the best he could do was to get the resident transferred to another surgical team without any acknowledgement of what had happened.
It was hardly a good result, but I never forgot that when institutional forces were trying to silence me, someone in authority believed me and fought for me.
Women who experience breastfeeding complications are no longer willing to go along with the testimonial silencing — erasure, refusal to believe, pathologizing, claiming “lack of support” disparaging women’s stories and banning from social media feeds — at the hands of breastfeeding professionals.
I hope they know that I believe them and will continue to fight for them.