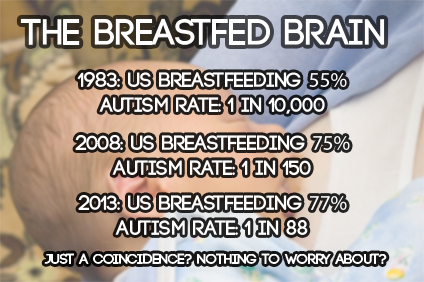
They say a picture is worth a thousand words and the images above and below are quite impressive. They compare the rate of autism over time compared to the rate of breastfeeding over time:

Over the past 4 decades, there has been a shocking rise in the prevalence of autism. Antivax activists have pointed out that there has been an increase in the number of vaccines that infants receive and conclude that vaccines cause autism. But as this graph shows there has also been a dramatic increase in breastfeeding rates. Indeed the two seem to rise in concert over time demonstrating a link between breastfeeding and autism.
Obviously more research is needed. We should be urgently investigating whether breastfeeding causes autism. We should reconsider recommendations designed to encourage breastfeeding and ask if we are ignoring the harmful effects. In the meantime, we should direct lactation consultants, La Leche League and the Baby Friendly Hospital Initiative to inform new mothers of the very clear association between breastfeeding and autism. How can women make an informed decision about breastfeeding if they don’t know about the link?
If you read this far you’re probably asking yourself what has happened to my reasoning abilities. Just because two phenomena rise in concert doesn’t make them linked. Sure, it raises the possibility, but it is grossly irresponsible for any medical professional or organization to announce a link based merely on a temporal association. I must be joking, right?
Sadly, I’m merely copying the efforts of the American Academy of Pediatrics to pressure women into breastfeeding. Their latest attempt to manipulate women, Breastfeeding and the Use of Human Milk was published earlier this week.
The press release highlights the disingenuous tactics:
Research has shown that breastfeeding is linked to decreased rates of lower respiratory tract infections, severe diarrhea, ear infections and obesity. Breastfeeding is associated with lower risk of sudden infant death syndrome, as well as other protective effects.
Notice that the authors do not — indeed CANNOT — say breastfeeding causes these benefits. They’re simply “linked” and “associated” with breastfeeding in EXACTLY THE SAME WAY rising rates of autism are “linked” and “associated” with breastfeeding.
The AAP paper continues:
There are continued benefits from breastfeeding beyond 1 year, and up to 2 years especially in the mother. Long-term breastfeeding is associated with protections against diabetes, high blood pressure, and cancers of the breast and ovaries.
The second sentence makes it clear that the first sentence is a falsehood. Long-term breastfeeding is merely “associated” with these benefits, NOT caused by them. In EXACTLY THE SAME way rising rates of autism are “associated” with extended breastfeeding.
I don’t for a moment believe that breastfeeding causes autism and neither should you. For the EXACT SAME reason, no one should yet declare that breastfeeding causes the “linked” and “associated” benefits touted by the AAP.
What’s really going on here?
Breastfeeding in industrialized countries is highly socially patterned. Breastfeeding and extended breastfeeding are far more common among women of higher education levels and higher socio-economic status. The purported “benefits” of breastfeeding are almost certainly benefits of wealth and access to health insurance and healthcare.
What does the scientific evidence really show?
The paper Is the “breast is best” mantra an oversimplification? is a comprehensive summary of the existing evidence and demonstrates that the benefits of breastfeeding have been overstated and the risks ignored.
The evidence for infant breastfeeding status and its association with health outcomes faces significant limitations; the great majority of those limitations tend to overestimate the benefits of breastfeeding. Nearly all evidence is based on observational studies, in which causality cannot be determined and self-selection bias, recall bias, and residual confounding limit the value or strength of the findings.
How is the average mother to understand the real benefits of breastfeeding (if there are any) when even the AAP is attempting to pressure them? Look at the actual wording of the claims.
When anyone tells you that breastfeeding is “linked to” or “associated with” myriad benefits remember that breastfeeding is ALSO “linked to” and “associated with” rising rates of autism.
Unless and until there is research to show that breastfeeding CAUSES a specific benefit, NO ONE — especially the AAP — should claim that it does. The touted “benefits” of breastfeeding are likely the result of higher socio-economic status, NOT breastfeeding itself.