A little more than a week ago I pondered why the American College of Nurse Midwives has thrown ethics to the wind by supporting waterbirth although it has been shown to be deadly. It is one example of the way in which CNMs value their professional autonomy over scientific evidence.
Now comes another in, of all places, the Journal of Midwifery and Women’s Health. Three CNMs have written an extraordinary paper that demonstrates far more powerfully than I ever could that CNMs reject science based standards that might limit their autonomy, as if science based standards are somehow discretionary. The paper is Formulating Evidence-Based Guidelines for Certified Nurse-Midwives and Certified Midwives Attending Home Births by Cook, Avery and Frisvold.
The study was simple and straightforward:
Following a review of home birth guidelines from multiple countries, a set of home birth practices guidelines for US CNMs/CMs was drafted. Fifteen American Midwifery Certification Board, Inc. (AMCB)-certified home birth midwives who participate in the American College of Nurse-Midwives (ACNM) home birth electronic mailing list considered the use of such a document in their practices and reviewed and commented on the guidelines.
In other words, the authors compiled evidence based standards that guide the practice of homebirth midwifery in countries like the Netherlands, the UK, Australia and Canada.
The response of the CNM reviewers was horrifying:
The primary concern expressed was that an adoption of national guidelines could compromise provider autonomy.
Apparently the CNMs favored the implementation of evidence based standards for American homebirth until they saw what the evidence showed. When they learned they were not practicing in accord with international evidence based homebirth standards, they decided to ditch the standards instead of changing their practice.
That, in a word, is unethical.
What were these international standards that CNMs rejected and where did those standards come from?
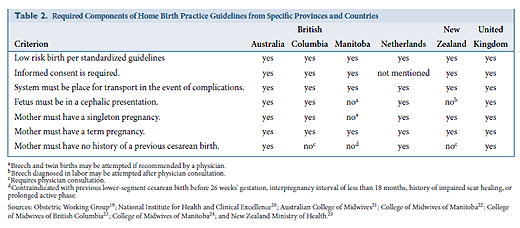
Five countries with provincially or nationally promulgated home birth midwifery guidelines met these criteria: Australia, Canada, the Netherlands, New Zealand, and the United Kingdom. Published guidelines of these countries were then reviewed for common themes. The following criteria for planning a home birth emerged: determination of low-risk pregnancy, informed consent, hospital transfer if complications arise, singleton pregnancy, fetus in the cephalic presentation, no history of previous cesarean birth, and term pregnancy.
Then:
After collection, review, and summary of these international guidelines, the primary author synthesized the information into draft home birth guidelines that could be used by US CNMs/CMs. The resulting 10-page document (see Supporting Information: Appendix S1) includes recommendations about licensure, physician collaboration, hospital transports, informed consent, documentation, client screening, equipment, medications, birth assistants, routine care of the mother and newborn, and emergency care of the mother and newborn
Five different countries; agreed upon basic standards for care… rejected by the CNM reviewers.
Even the authors were shocked:
… [T]he authors were surprised that the reviewers expressed greater interest in developing and implementing national home birth midwifery guidelines prior to reviewing the proposed guidelines versus after their review…
The primary concern raised by the reviewers was whether or not guidelines would impact their autonomy. Guidelines are intended to provide best practices from which providers can meet individual client needs but also discourage providers from diverging from safe practices. The reviewers specified that the proposed guidelines might not support them if they choose to attend the home birth of a woman with a breech presentation or a twin gestation or a woman who desires a trial of labor after a previous cesarean. While CNMs/CMs attending home births may have the skill to attend such births, the safety net available in an institutional setting is advantageous and may be preferable for such births…
Indeed, the authors feel compelled to re-state the obvious requirement for ethical practice:
Although ensuring client safety may at times conflict with provider and client preferences, safety is the first priority for improving the quality of health care.
Apparently not for CNMs.
The authors note:
Fundamental to international home birth guidelines that were examined in this project is a distinction between low risk and high-risk maternity criteria. Normal birth has been defined in a joint statement by the Society of Obstetricians and Gynaecologists of Canada; the Association of Women’s Health, Obstetric, and Neonatal Nurses of Canada; the Canadian Association of Midwives; the College of Family Physicians of Canada; and the Society of Rural Physicians of Canada as spontaneous labor with a singleton fetus in a
vertex presentation at 37 to 42 weeks’ gestation after an uncomplicated pregnancy. This definition is consistent with the World Health Organization definition and the UK Maternity Care Working Party definition supported by the RCOG and RCM. (emphasis in original)
We already know that American homebirth midwives (CPMs, LMs, DEMs) lack basic professional ethics. Now comes stunning confirmation that American CNMs attending homebirths are equally ethically bankrupt.
What should American women take away from this study?
It is yet more evidence that midwives who attend homebirths (CPMs and CNMs) value their professional autonomy over whether your baby lives or dies. It is more important for them to maintain control over you (and collect a fee from you) than to accurately advise you. Moreover, the homebirth safety data from countries like the Netherlands and the UK can’t possibly apply to homebirth in the US because even homebirth CNMs refuse to follow the guidelines that govern homebirth in those countries.
Homebirth is a fringe practice. We can argue about whether it might be safe under ideal conditions, but it CANNOT be safe in the US because the midwives who attend homebirths (CPMs and CNMs) explicitly reject safety standards. And as long as they continue to do so, babies (and sometimes mothers) will continue to die preventable deaths at their hands.