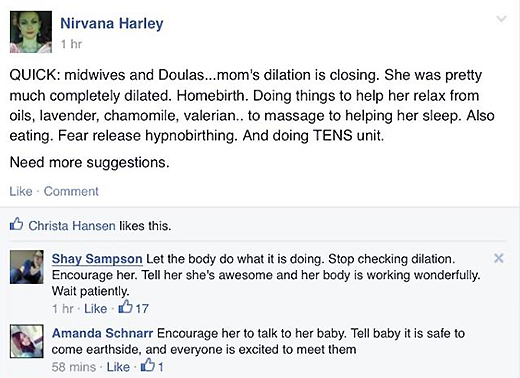
How many babies have to die before homebirth advocates acknowledge that it has become an act of selfishness? How about two babies a day?
Last Sunday, the same day that doula Nirvana “Harley” Jennette was taking hideous risks with the life of a baby in Georgia, two other midwives (one in Texas, and one in Oregon) tooks hideous risks with the lives of two additional babies and both babies sustained fatal injuries as a result. It seems that “trusting birth” is just a euphemism for “letting babies die preventable deaths.”
Let’s be honest here. Homebirth midwives are under tremendous pressure to keep their clients at home. If they have to transfer to the hospital during labor, it’s because they misjudged the situation. They may be exposed to disciplinary or even legal action. And the longer they wait to transfer, the more likely it will be that the baby suffers a fatal injury, so the more likely they are to face dire consequences for themselves. Paradoxically, the more dangerous the situation becomes (and, therefore, the more likely that the homebirth midwife will face scrutiny), the more pressure she feels to stay at home and just hope against hope for a happy outcome.
That’s how babies in Portland and in Dallas-Fort Worth sustained their fatal injuries.
The mother in Portland was expecting her first baby. Membranes had been ruptured for more than 40 hours. Labor was protracted but not out of the bounds expected for a first labor and the baby was delivered and did not breathe.
The midwives waited 15 minutes to call for assistance, and the baby did not reach the hospital for over an hour after her birth.
On admission to the hospital, she was profoundly acidotic, a sign of long term lack of oxygen. Despite cooling therapy, she had suffered a catastrophic brain injury, so severe that baby has been taken home to die.
Yet again, another utterly clueless midwife is shocked to catch a nearly dead baby. The time required for transfer should give pause to any homebirth advocate who thinks they can get to the hospital fast enough in an emergency. The baby needed the immediate attention of a neonatologist when she was born. Instead, she didn’t arrive at the hospital until over an hour later. And all that time even more of her brain cells were dying. The baby did not have to sustain a catastrophic brain injury. She was not “meant” to sustain a catastrophic brain injury. It happened because her mother gambled the baby’s life in exchange for a birth “experience” and the baby lost.
Baby James sustained his fatal birth injury while his mother was attempting a home VBAC. She had had a C-section in her first pregnancy, and a successful hospital VBAC in her second. She was an excellent candidate for a hospital VBAC. No one is ever a candidate for a home VBAC.
James died of an abruption that his mother’s student midwife failed to recognize despite heavy vaginal bleeding. Where was the actual midwife? Reportedly she was home resting because the mother’s labor was so long. That, of course, was the first sign of imminent disaster. A woman who has had a successful VBAC should not be experiencing a prolonged labor subsequently. Indeed, the prolonged labor, with the accompanying possibility that the baby did not fit, dramatically raised the risk of uterine rupture. An abruption during an attempted VBAC is often the result of rupture of the uterus, but I have not been able to ascertain whether James’ mother experienced a ruptured uterus as well as an abruption.
I did receive information that was reportedly posted by the student in a student homebirth midwifery group. According to that information, the student midwife called her preceptor at home to tell her about the excessive bleeding, and was reassured that it was fine. I was told that it was ultimately the father who called 911 because the student wouldn’t. Unfortunately, it was too late. An emergency C-section was performed, but James had sustained catastrophic brain damage and was removed from life support 18 hours later. James was not “meant” to suffer a catastrophic brain injury. It happened because his mother chose homebirth.
The poor baby’s obituary is appalling. Indeed it appears as if the student midwife wrote it:
When the time came for him, his mama labored mightily to bring him into this world and his daddy was so proud of his mama. He lived for 18 wonderful hours…
Wonderful hours? I doubt those hours were wonderful for either James or his parents.
Survivors: Mama and daddy; sisters; grandparents … and midwife Kaitlyn Wages loved this boy and his family more than words can say.
A baby is dead and the obituary talks about his mother’s “performance” in labor and how much the student midwife loved him?
The midwives have written extensively about the baby:
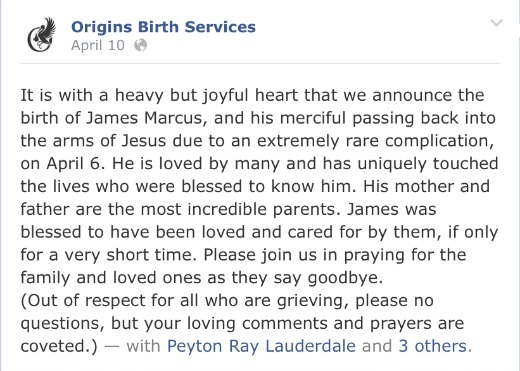
An extremely rare complication? No, abruption is a common complication, occuring in 0.4-1% of all pregnancies.
No questions?
I asked the midwives on their Facebook page why this baby died. Their response? To delete the question and ban me. I wonder if that had anything to do with concealing potential culpability from their other clients.
Why shouldn’t ask questions of people who are grieving?
It may not be the time to ask questions of the parents, but it is most certainly the time to ask questions of the midwives. This is the time for a full investigation into a neonatal death that appears to have been entirely preventable.
The sad fact is that these deaths are not remotely surprising. Giving birth at home is equivalent to leaving your infant at home alone. In both cases, the mother is “trusting” that the chance of anything going wrong is small enough that it’s okay if she puts her own experience first. In fact, leaving your infant home alone while you got out and party is probably safer than choosing homebirth. The odds that the baby will experience a life threatening complication while sleeping (or screaming and crying) at home is vanishingly small. The odds that your infant will experience a life threatening complication at homebirth is thousands of times higher. So if going out partying and leaving your infant behind is grossly irresponsible, that makes choosing a homebirth more irresponsible still.
The bottom line is that giving birth in a hospital is an act of love. With the mounting evidence that American homebirth is far more dangerous than we ever imagined, giving birth at home has become an act of selfishness.