One of the biggest problems in American homebirth is that homebirth midwives don’t know what they don’t know. Their background in obstetrics, science and statistics is very limited; so limited, in fact, that they have no idea how little they know compared to those who have far more education and training in these subjects. The tendency to overestimate their knowledge and abilities is called as the Dunning-Kruger effect.
The classic paper on this phenomenon is Unskilled and Unaware of It: How Difficulties in Recognizing One’s Own Incompetence Lead to Inflated Self-Assessments published in the Journal of Personality and Social Psychology in 1999. The paper reports on a variety of experiments that were used to evaluate individuals’ actual performance compared to predicted performance.
For example, study subjects were given a test of basic logic:
[pullquote align=”right” color=”#c9defd”]Those who know the least are also the least capable of understanding how little they know.[/pullquote]
…Participants … completed a 20-item logical reasoning test that we created using questions taken from a Law School Admissions Test (LSAT) test preparation guide. Afterward, participants … compared their “general logical reasoning ability” with that of other students from their psychology class by providing their percentile ranking. Second, they estimated how their score on the test would compare with that of their classmates, again on a percentile scale. Finally, they estimated how many test questions (out of 20) they thought they had answered correctly…
The results are displayed in the following graph:
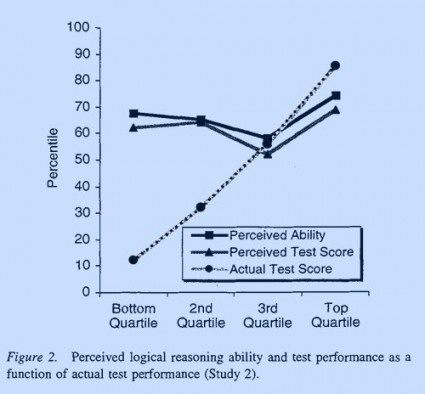
The dark lines represent the test subjects’ rating of their logical reasoning ability and the score they predicted they would get. The dotted line represents the actual score. The graph demonstrates that the ability to correctly predict one’s score is directly related to the actual score. Those who scored poorest on the test of logic grossly overestimated their ability; those who did slightly better slightly overestimated their performance; and those who scored moderately well were accurate in predicting their own performance.
In other words, those who knew the least were also the least capable in understanding how little they knew.
The authors also found that improving the subjects knowledge of logic led to more realistic personal assessments. They divided a new group of test subjects in two. One half received a lesson in logic before the test; the other half received a lesson in an unrelated subject. Those who received the lesson in logic were much more likely to accurately predict performance on the test.
… Before receiving the training packet, these participants [in the lowest quartile] believed that their ability fell in the 55th percentile, that their performance on the test fell in the 51st percentile, and that they had answered 5.3 problems [out of 10] correctly. After training, these same participants thought their ability fell in the 44th percentile, their test in the 32nd percentile, and that they had answered only 1.0 problems correctly…
No such increase in calibration was found for bottom-quartile participants in the untrained group.
As the authors explain:
Participants scoring in the bottom quartile on a test of logic grossly overestimated their test performance — but became significantly more calibrated after their logical reasoning skills were improved. In contrast, those in the bottom quartile who did not receive this aid continued to hold the mistaken impression that they had performed just fine.
Why hadn’t the study participants realized their own deficiencies in basic logic simply by interacting over the course of their lifetime with other people who knew more basic logic?
… [S]ome tasks and settings preclude people from receiving self-correcting information that would reveal the suboptimal nature of their decisions. [And], even if people receive negative feedback, they still must come to an accurate understanding of why that failure has occurred.
That’s why homebirth midwives have no idea how little they know. Because homebirth midwives never encounter anyone in their training besides other homebirth midwives, they have no opportunity to observe that many other health professionals have a much larger knowledge base and a much greater skill set. When disasters occur at homebirth, midwives fail to understand that they were responsible and simply dismiss tragedies with the all purpose adage that “some babies die.”
Moreover:
… [I]ncompetent individuals may be unable to take full advantage of one particular kind of feedback: social comparison. One of the ways people gain insight into their own competence is by watching the behavior of others… However, [our study] showed that incompetent individuals are unable to take full advantage of such opportunities. Compared with their more expert peers, they were less able to spot competence when they saw it, and as a consequence, were less able to learn that their ability estimates were incorrect.
This problem is greatly aggravated in homebirth midwifery because homebirth midwives are literally taught to view anyone who does things differently as objects of contempt. Doctors are supposedly greedy, incompetent and ignore scientific evidence. This attitude is best illustrated by the perjorative appellation of certified nurse midwives as “medwives.” Though CNMs have far more education and training than homebirth midwives, homebirth midwives prefer to pretend that CNMs spent that extra time being “socialized” (i.e. brainwashed) in “techno-medicine.”
The authors conclude:
… [W]e present this article as an exploration into why people tend to hold overly optimistic and miscalibrated views about themselves. We propose that those with limited knowledge in a domain suffer a dual burden: Not only do they reach mistaken conclusions and make regrettable errors, but their incompetence robs them of the ability to realize it.
Similarly, homebirth midwives hold overly optimistic views about their knowledge base and their clinical skills. Not only do they reach mistaken conclusions and make deadly errors, but their incompetence robs them of the ability to understand just how incompetent they are.
This piece first appeared in January 2011.