I have not forgotten about Gavin Michael and our efforts to hold midwives Christy Collins and Jan Tritten accountable for the preventable tragedy of his death. I have been in correspondence with his parents and they are currently determining how best to proceed. It may take some time, especially since they are still reeling from the loss of their baby.
Gavin Michael’s story is in many ways all too familiar to those of us struggling to educate the public about the increased risk of death at homebirth. A mother choose homebirth because she thinks she is making a safe and loving choice for her baby. Other medical professionals point out the risks, but the mother does not take them seriously. Family and friends express their worry and concern, but the mother assures them that she knows what she is doing. The situation grows steadily worse, either because a pregnancy complication is being neglected, or because a stalled or ineffective labor is being ignored. Ultimately the baby is injured or dies, even though this is the last thing that the mother imagined or wanted to happen.
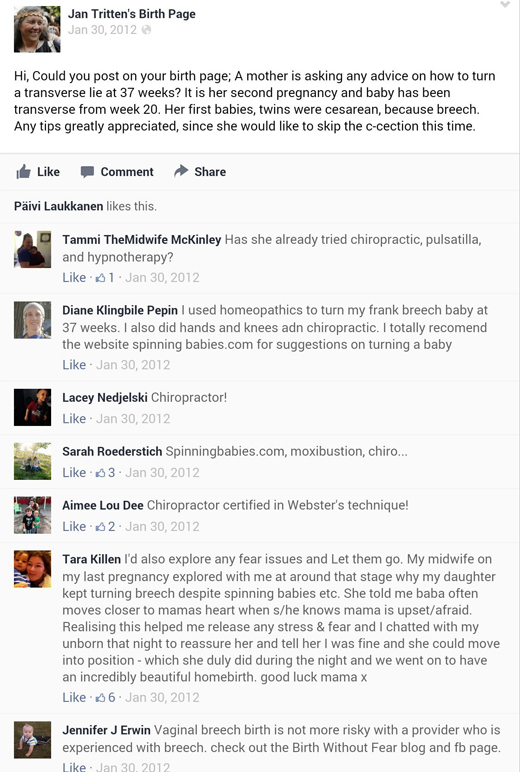
The death of baby Gavin is chilling in a myriad of ways, especially because his struggle to survive played out in real time on Facebook. One aspect that I find particularly chilling is illustrated by this quote from Christy Collins apparently written in response to Gavin’s death.
Instead of … telling you to “be prepared that the perinatologist doing the NST is likely to tell you that your baby could die if he doesn’t come out;” those should have been MY words.
It’s chilling because in one sentence Collins captures the emotional dependency that she and other homebirth midwives strive to induce in their clients. Collins deliberately cut Gavin’s mother off from any medical personnel who might have helped her or Gavin by inducing such profound distrust that even if a doctor looked Gavin’s mother in the eye and told her that her baby was in imminent danger of death, she had been carefully coached in advance to reject medical advise that was both excellent and true.
I have written in the past that homebirth advocacy bears many of the hallmarks of a cult. It creates almost religious devotion to the philosophy of homebirth, places birth at the level of a deity by constant reminders to “trust birth” and demands sacrifice from acolytes, in both pain and potential injury to the baby. The most cult like aspect, however, is the emotional dependence that homebirth midwives strive to induce in their clients.
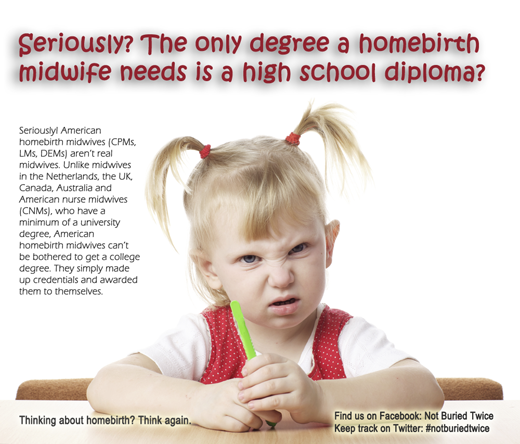
It’s no secret that 100% of the income of homebirth midwives comes from homebirth. But the economic motivation is only one factor in the determination of untrained lay people to masquerade as “midwives” even though they cannot be bothered to get a real midwifery degree. Providing medical care is not the goal for a homebirth midwife; gaining emotional power over and adulation from clients is an equally powerful goal.
The blueprint of midwife manipulation appears to be this:
To maintain your power you must always be needed and wanted. Make women depend on you and only you. To do that, you must convince the client that medical professionals are ignorant and only want to hurt her and her baby. You must explain ahead of time exactly the medical advice that these professionals will give so she will be prepared to ignore it. You must also work assiduously to isolate the client from her family and friends, emphasizing that their apparent concern is just a reflection that they are not as “educated” as she is. Makes her self-esteem utterly dependent on your approval, for the moment she trusts someone other than you, your power over her is ended.
Consider this explanation of emotional dependence and how to create it*:
Inducing Emotional Dependence
People become emotionally “hooked” on those persons who can truly satisfy their never-ending need for human understanding. The key … is to first get that person to become emotionally dependent on you… As you learn to satisfy a person’s deep-rooted emotional need for understanding, you will in time find them becoming emotionally dependent on you.
- Be There (In Person)!
- Listen Reflectively
- Avoid Being Critical
- Express Genuine Admiration And Praise
- Supply Sympathy
It sounds like a primer for homebirth midwives, doesn’t it? Hence the hour long appointments for prenatal visits, the careful nurturing of the “friendship” between midwife and client, and the endless infantilizing praise — You are so educated! You are powerful, mama! You are a birth warrior goddess!
It’s all carefully constructed (though not necessarily consciously) to make the mother emotionally dependent on the midwife and likely to look to her for everything — medical advice, guidance, praise, support, self worth.
But like any serious attempt at inducing emotional dependence, it doesn’t rest solely on the positive. Destroying trust in others is key to maintaining emotional control. Hence it is critically important to demean modern obstetrics (“not evidence based”) and obstetricians (“they recommend C-sections only for money and convenience”) at every turn. Whether consciously or unconsciously, homebirth midwives recognize that obstetricians know far more about pregnancy and childbirth than homebirth midwives do. Therefore, it is imperative to make sure that the mother is kept as far as possible, both physically and emotionally, from real medical professionals. To that end, the midwife must be the gatekeeper between the mother and obstetricians. Only the midwife can decide whether and when the services of an obstetrician and hospital are needed. Until that moment, all her persuasive power will be bent toward keeping the mother at home.
The homebirth midwife understands (consciously or unconsciously) that the mother’s reliance on her family and friends for comfort and support threatens the exclusive power relationship that the midwife is seeking. Hence the midwife is always working to marginalize and create distrust of parents, in-laws and friends who can supplant her. They are marginalized by pointing out their lack of “education,” their culturally determined “fear of birth,” and their pathetic submission to authority figures. When all else fails, the homebirth midwife moves to have family and friends excluded from the birth itself, and in extreme situations, will physically isolate the mother and refuse entry to all others.
Christy Collins appeared to play that role to perfection in her relationship with Gavin’s mother. She even used the midwife’s trump card, the “dead baby card” to inoculate Gavin’s mother against the possibility of listening to an obstetrician. Every homebirth midwife knows that a mother will do almost anything to prevent the death of her baby. Since Christy understood that a doctor would tell Gavin’s mother that her baby might die, as zero amniotic fluid is indeed a sign of impending death, Christy prepared the mother in advance to ignore his counsel.
Christy knew that Gavin might die. She understood both that a doctor would tell that to Gavin’s mother and that it would be true. Inevitably she would lose emotional and physical control of Gavin’s mother, who would turn to an obstetrician, so she neutralized that possibility in advance by deriding the warning as the “dead baby card.”
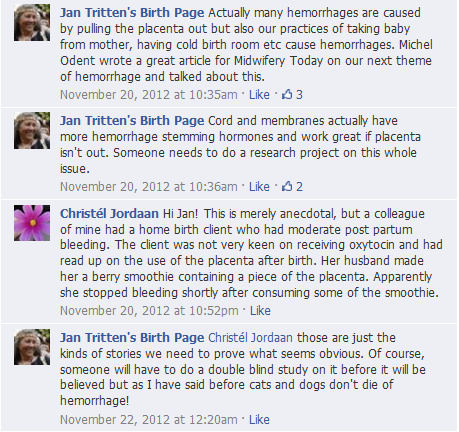
Then Christy approached Jan Tritten, in her role as Editor of Midwifery Today, to gain support for her desire to risk Gavin’s life in order to maintain control over Gavin’s mother. Surely Gavin’s mother would go into labor soon, right? Surely Gavin would survive until then, right? Or maybe Jan and her Facebook friends might think of a way to induce labor without requiring Christy to give up emotional control of the mother. It apparently never occurred to Jan Tritten to tell Christy to place the baby’s well being over her own emotional needs. In my view, Tritten’s failure to warn Christy wasn’t merely buffoonish ignorance on Tritten’s part; it was implicit recognition and acknowledgement of the “real” task at hand, maintaining emotional control over Gavin’s mother even if at the cost of Gavin’s death.
Homebirth midwives are not medical professionals. They are laypeople who, to fulfill their own emotional needs, masquerade as “midwives,” allowing them to create emotional dependence and worship in mothers. That’s why medical knowledge is irrelevant for them. It’s not about babies and it’s not about safety. Homebirth midwifery is about homebirth midwives, and their need for power, control and adulation. Babies who die are nothing more than unavoidable, though regrettable, collateral damage.
*The explanation and list comes from a website that purports to teach people how to make others love them.