The largest, most comprehensive study ever done of homebirth has released its results and there’s nothing left to argue about: homebirth increases the risk of perinatal death.
The Birthplace Study, a large multi-year study, was designed to address the safety of place of birth by controlling for the many factors that had not been handled properly in other studies. The study looked at intended place of birth to rule out improperly assigning transferred patients to the hospital group, and included only the lowest possible risk women. The study was conducted by The National Perinatal Epidemiology Unit in the United Kingdom.
The authors found that homebirth increases the risk of death, brain damage and serious neonatal injury.
The authors chose to evaluate the results by creating an index of primary events comprising intrapartum stillbirths, early neonatal deaths, neonatal encephalopathy [brain damage] meconium aspiration syndrome, brachial plexus injury, and fractured humerus or clavicle. Using this measurement:
… [T]here was a significant excess of the primary outcome in births planned at home compared with those planned in obstetric units in the restricted group of women without complicating conditions at the start of care in labour. In the subgroup analysis stratified by parity, there was an increased incidence of the primary outcome for nulliparous women in the planned home birth group (weighted incidence 9.3 per 1000 births, 95% confidence interval 6.5 to 13.1) compared with the obstetric unit group (weighted incidence 5.3, 3.9 to 7.3).
In other words, the risk of death and serious injury was approximately double in the homebirth group and that increase was seen mainly among first time mothers.
The authors did not include the number and distribution of specific primary events within the paper itself, but did publish a 78 page supplementary file including this information. The following tables are adapted from that file. (OU stands for Obstetric unit [hospital], AMU stands for along side maternity unit [in hospital birth center], and FMU for free-standing maternity unit [independent birth center].)
Stillbirths

Early neonatal deaths (to 7 days)

Encephalopathy [brain damage]
The authors put the best possible face on the outcome:
… Adverse perinatal outcomes are uncommon in all settings, while interventions during labour and birth are much less common for births planned in non-obstetric unit settings. For nulliparous women, there is some evidence that planning birth at home is associated with a higher risk of an adverse perinatal outcome…
What can we conclude?
Homebirth increases the risk of perinatal death and brain damage in the lowest risk women receiving care from highly trained midwives (often two) and liberal access to transfer.
Homebirth increases the risk of perinatal death and brain damage even when, at the start of labor, breech, twins, VBAC. positive GBS status, gestational diabetes and obesity were excluded. All routinely occur at homebirths in the US, the UK and Australia.
And how about the purported “risks” of interventions that homebirth advocates are always taking about?
Homebirth increases the risk of perinatal death and brain damage even though the incidence of epidural use was 5 times higher in the hospital group.
Homebirth increases the risk of perinatal death and brain damage even though the incidence of pitocin augmentation was 5 times higher in the hospital group.
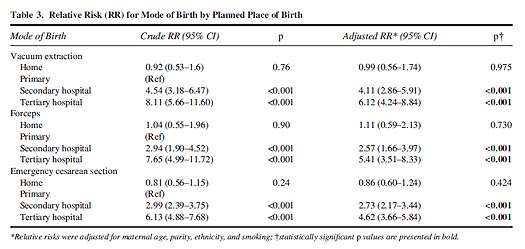
Homebirth increases the risk of perinatal death and brain damage even though the incidence of operative vaginal delivery was 3-4 times higher in the hospital group.
Homebirth increases the risk of perinatal death and brain damage even though the C-section rate was 4 times higher in the hospital group.
In other words, any way you choose to look at it, no matter how carefully you slice and dice the data, there is simply no getting around the fact that homebirth increases the risk of perinatal death and brain damage.