When I was in elementary school, this was a popular riddle:
A plane crashed on the exact border between the US and Canada. Where did they bury the survivors?
Much hilarity ensued after various guesses since you don’t bury survivors. Only those who died are buried.
I am reminded of that riddle when I read quack claims about the “superiority” of natural immunity.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Vaccine immunity is superior to natural immunity because there are dramatically more survivors of the disease itself.[/pullquote]
Why?
It is axiomatic among anti-vax quacks that natural immunity is superior to vaccine produced immunity.
Quaxpert Andrew Wakefield insists in regard to measles:
Measles vaccine has destroyed natural Herd Immunity and replaced it with a temporary and inadequate quasi Herd Immunity that necessitates a dependence on vaccination …
According to NaturalNews clown Mike Adams:
There is only one kind of immunity and that is natural immunity which is achieved by battling the infectious diseases itself. Vaccination is merely the artificial triggering of temporary responses to manmade pathogens…
Both Wakefield and Adams seem to think that the relevant issue is what happens to survivors. Indeed, in some cases, natural immunity among survivors can be more robust that vaccine induced immunity. If faced with a second outbreak of the disease, those who got the disease the first time may have superior immunity to those who were vaccinated against it and therefore missed it entirely. That is supposed to “prove” the purported superiority of natural immunity.
But just like the question about burial is the red herring in the elementary school riddle, the focus on post disease immunity is a red herring in the quack claims. Highlighting the immune status of survivors deliberately misses the point. Vaccine immunity is superior to natural immunity because there are dramatically more survivors of the disease itself.
History offers many examples of this basic fact. Approximately one third of the Eurasian population (75-200 million) succumbed to the Black Death in the mid 1300’s. No doubt the survivors had robust immunity to the particular strain of Yersinia pestis that was circulating at the time. A vaccine against plague, had it existed, might have resulted in less robust immunity among survivors but there would have been tens of millions of more survivors.
More recently, the Spanish flu epidemic in 1918 afflicted approximately 500 million people and killed 50-100 million of them. Perhaps the people who survived had more robust immunity to the particular strain of influenza thereafter than a vaccine, had it existed, would have provided. But if a vaccine had existed, a substantial proportion of the 50-100 million who died would have survived.
Our experience with vaccinations makes the point even more dramatically.
Consider this CDC chart created in the early years of the anti-vax movement:
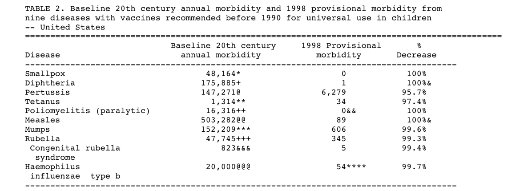
The results are extraordinary:
Vaccine immunity led to the extinction of smallpox, a feat that natural immunity never even approached.
Cases of such “mild” childhood diseases as pertussis dropped from more than 147,000 per year to less than 7,000. Annual measles cases dropped from more than 503,000 to less than 100. Diphtheria, polio and congenital rubella nearly disappeared. And if you don’t get the diseases, you can’t die from the diseases, can’t be rendered paralyzed, blind or deaf by the diseases.
The difference between vaccine immunity is the difference between prevention and treatment … and prevention is always superior.
Insisting that the purported superiority of natural immunity among survivors means that vaccines are unnecessary makes as much sense as insisting that diet and exercise are unnecessary to prevent heart disease because most survivors won’t go on to have a second heart attack. You have to survive the first attack for any concerns about a second heart attack to be relevant. Similarly, you have to survive pertussis, measles, polio, diphtheria or smallpox in order for your immune status thereafter to be relevant.
There is no question that vaccine immunity is superior because vaccine immunity saves millions of lives that cannot be saved by natural immunity. And that would be obvious if anti-vax quacks and charlatans weren’t so effective at distracting lay people with red herrings like the immune status of survivors.