
There seems to be a great deal of confusion among natural childbirth and homebirth advocates about the nature and treatment of vaginal tears.
All vaginal tears are not alike. The decision on whether they should be repaired, how they should be repaired and the consequences of not repairing them depend completely on the type of tear. Unfortunately, the need for repair is negatively correlated with the ability of a midwife to repair it. In other words, homebirth midwives know how to repair only minimal tears that would probably heal without repair. Most midwives, including certified nurse midwives, do not know how the to repair the tears that are most critical to repair. These are the tears that lead to bowel incontinence.
Most tears occur downward into the area between the vagina and rectum known as the perineum. It is more accurate, therefore, to refer to them as perineal tears. The Mayo Clinic website has an excellent series of slides detailing the normal anatomy of the perineum and the 4 degrees of perineal tears.
The illustration below portrays the normal perineal anatomy.

The perineal muscles identified in the illustration are the superficial perineal muscles; there is another deeper set that is more important for holding the pelvic organs in place. The anal sphincter is the ring of muscle that holds the anus closed. It is directly responsible for preventing bowel incontinence. If it will is torn completely apart and not properly repaired, the woman will be incontinent. Of note, this form of incontinence is different from a fistula, which is a hole inside the upper vagina that connects it directly to the bladder in front, the bowel behind or both.
Perineal tears are graded in severity from first degree to fourth degree, with first degree being minor and fourth degree most severe.
You can see a first degree tear below.
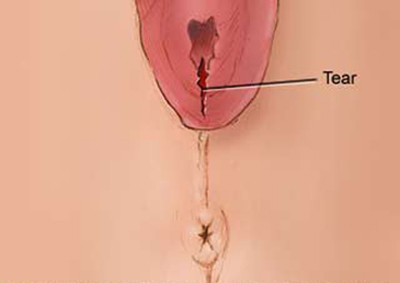
The tear is superficial and therefore minor. It’s the equivalent of a paper cut, and like a paper cut, will heal without stitches. Some people even think they heal better without stitches. First degree tears are very common.
Second degree tears are also common, but they heal better when stitched back together.
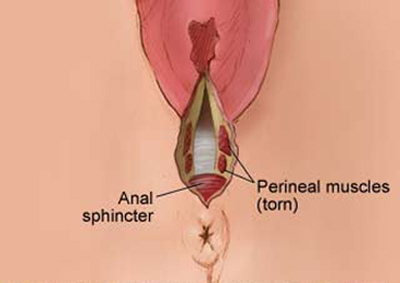
As you can see, this tear extends into the muscles that surround the vagina. The tear can be short in length or it can extend the entire distance between the bottom of the vagina and the top of the anal sphincter. A median episiotomy produces a second degree tear like this.
Putting the muscles back together makes sense if you want to preserve the natural shape and anatomy of the vagina. If it is not repaired, the opening to the vagina will gape, but there are usually no serious consequences of failing to repair it. Theoretically it is possible that the muscles will be able to heal back together on their own, but it is extremely unlikely. With the exception of very tiny tears, there are no circumstances under which a second degree heals “better” if it is not stitched.
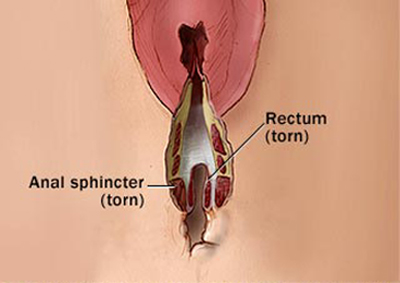
A third degree tear MUST be repaired, and you can understand why when you look at the illustration.

The anal sphincter has been torn apart. If it is not repaired, bowel contents will be allowed to flow freely out of the rectum and there is nothing a woman can do to prevent it. Moreover, if the anal sphincter is not repaired at the time of delivery, the repair itself becomes much more complicated.
Unfortunately, though the illustrations make the difference between a second degree and third degree tear obvious, it is usually not so clear in real life. That’s because the muscle fibers of the anal sphincter tend to retract back into the surrounding tissue. If that happens, a third degree tear looks exactly like a second degree tear. If a tear extends the entire length of the perineum, the only way to tell the difference between a second degree and third degree tear is to put a finger in the anus and feel if the sphincter is still present.
A torn sphincter will not heal itself because the torn ends are usually far apart from each other after the muscle fibers retract. The superficial layers of the tear will heal and it may look like everything is normal, but the woman will not be able to control her bowel function and will definitely need an involved surgical repair under anesthesia.
Most midwives do not know how to repair a third degree tear and most homebirth midwives don’t even know how to tell the difference between a second degree tear and a third degree tear. Therefore, they often fall back on the tried and true tactic that homebirth midwives use when confronted with something they cannot do; they insist that it is unnecessary. In the case of perineal tears, this has the paradoxical effect that the more serious the tear, the more likely the homebirth midwife is to insist that it doesn’t need to be repaired.
The repair itself is not rocket science. You simply have to bring the torn ends of the sphincter out from the surrounding tissue and stitch them together. But you can only do that if you have the experience to diagnose the problem and carry the specialized clamps that will allow you to find and grasp the torn ends. Since homebirth midwives don’t have either, they often fail to repair third degree tears and the patient ends up with a surgical procedure under general anesthesia within months after the birth.
A fourth degree tear is the most serious. A fourth degree tear extends into the rectum. The result is that the vaginal and rectum form one continuous space.
The repair of a fourth degree tear starts with the repair of the rectum itself. Depending on the how far the tear extends up into the rectum, the repair can be technically challenging and can take an hour or more. Once the rectum is repaired, the rest of the tear is repaired like any other third degree tear. However, because the rectum itself has been torn, the possibility exists that the tear may heal improperly and leave a hole (fistula) between the vagina and rectum with consent leaking of feces from the vagina. Obviously, a fourth degree tear MUST be repaired in the immediate aftermath of birth.
Let’s review:
- Perineal tears are classified by severity.
- First degree tears do not need to be stitched.
- Second degree tears ought to be stitched but the results are not catastrophic if they are not stitched.
- Third and fourth degree tears MUST be stitched or the woman will be left with bowel incontinence.
- Third and fourth degree tears can only be diagnosed by someone with experience.
- Third and fourth degree tears will NOT heal by themselves.
- Third and fourth degree tears must be repaired by someone with extensive experience in repairing them.
Bedrest does NOT heal tears and the only thing it does is increase the risk of a woman developing a deep vein thrombosis or pulmonary embolus. If a homebirth midwives tells you that your tear will heal if you just stay on bedrest, it is a signal to get to the hospital as soon as possible for an expert diagnosis and repair. Otherwise, the results are likely to be embarrassing, painful, and require further more extensive surgery in the future.