
Dear Ms. Lake,
According to The New York Times:
One of the most talked about and provocative documentaries about childbirth is having its own rebirth.
“The Business of Being Born,” the 2008 film by the former talk show host Ricki Lake questioning the American medical system’s approach to childbirth and presenting the benefits of home birth, will be rereleased digitally in late January, becoming available globally for the first time. The updated version of the documentary, which also spawned a DVD series and a book, will include interviews with celebrities like the actress and model Stacy Keibler who were swayed by the film and, like Ms. Lake, gave birth at home.
I’ve noticed that you have been quick to claim credit for a rising number of homebirths:
The impact of the documentary was monumental. The blogosphere blew up (I can handle a few people yelling at me if it means my message is being heard!) Every day women stop me on the street to share stories of their safe, successful, meaningful births. Many say they felt “in the dark” about their options until seeing The Business of Being Born …
I wonder if you’re also willing to accept blame … for the babies and mothers who have died because they believed your nonsense.
What do you say when women stop you to share stories of their dead babies, babies who died because their mothers saw your movie and believe that homebirth was safe and empowering? What do you say when they share their stories of a ruptured uterus, a breech baby with a trapped head, a severe shoulder dystocia? What do you say when they tell you how their “midwife” encouraged them to labor for days and push for hours, all the while unaware that the baby had died from the stress of labor?
What do you tell them, Ms. Lake? How do you explain why you ignore the large and growing amount of data and statistics that show that homebirth leads to the preventable deaths of babies who didn’t have to die?
I know, and perhaps you know, too, that in January 2014 the Midwives Alliance of North America (MANA), the organization that represents homebirth midwives, published their landmark “study” (actually a non-representative survey of less than 30% of their members completed 5 years ago) claiming that homebirth is safe but ACTUALLY showing that homebirth increases the risk of perinatal death by 450%.

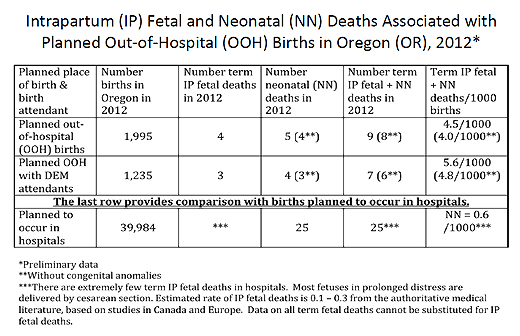
In March 2013, Oregon released an analysis of homebirth deaths prepared by Judith Rooks, CNM, MPH that showed that PLANNED homebirth with a LICENSED Oregon homebirth midwife had a death rate 800% higher than comparable risk hospital birth.
In June 2013, Grunebaum et al. demonstrated that homebirth increases the risk of a 5 minute Apgar score of zero by nearly 1000%.
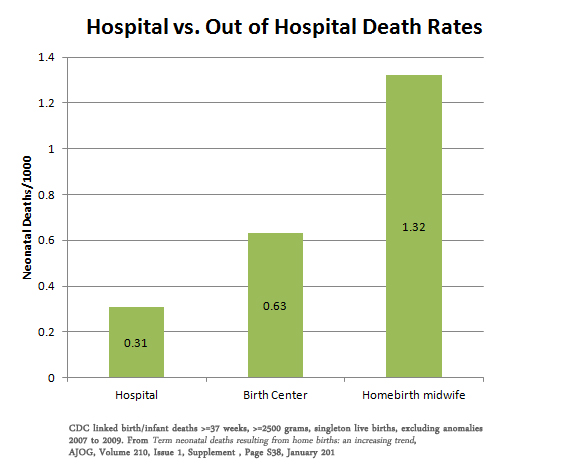
In February 2014, he presented data showing that homebirth has a 4X higher risk of neonatal death than comparable risk hospital birth:
In January of 2014, Wasden et al. demonstrated that the risk of anoxic brain injury is more than 18 times higher at homebirth than comparable risk hospital birth.
And those are just the highlights. Other papers and datasets were also published and all, without fail, showed that homebirth has a death rate 3-9 X higher than low risk hospital birth.
Let’s be honest, Ms. Lake, the homebirth industry ignores safety in order to make money and you are the leading example, as you mentioned in explaining why you made BOBB in the first place:
She said that she made the film because she was contemplating her legacy after the September 11th attacks, and that her only goal was not to lose money.
Indeed, you turned homebirth into an industry, both for yourself and others. There’s an entire industry of homebirth midwives [unlike real American midwives (CNMs), homebirth midwives (CPMs, LMs, DEMs, lay midwives lack the education and training of all other midwives in the first world], doulas, childbirth educators, birth pool rental services, etc. profiting by risking babies lives, and just like you, Ms. Lake, they take no responsibility for the death and destruction they leave in their wake.
Ms. Lake, you ought to set some of your profits from YOUR business of being born (books, DVDs, etc) into a no-fault compensation fund for those parents who have lost babies at a homebirth. I’m not sure how much money would be available for each family, since, unfortunately, there is a large and growing number of such families, and I don’t know if would be enough to cover the millions of taxpayer dollars that are going to be spent caring for the babies who were left brain damaged by homebirth. Nonetheless, it seems to me that it is the least you could do.
But if you don’t plan to take responsibility, and I’m not holding my breath because I would turn awfully blue, the very least you could do is amend your film, books and website to reflect the increased death rate of homebirth. I don’t doubt that you were unaware of the dangers of homebirth when you started, but you can’t be unaware now. It doesn’t take any specialized knowledge to count the growing number of dead babies, babies who died preventable deaths because their mother listened to you. But if you don’t correct the mistruths, half truths and outright lies in the original issue of BOBB, any money you make now is just blood money.
Sincerely (and with a great deal of sadness and anger),
Amy Tuteur, MD