
You might think these women would have more important things to worry about like the hideous death rates at their hands at Morecambe Bay (where 16 babies and 3 mothers died over a 9 year period) to the newly revealed horror at Royal Oldham/ North Manchester General Hospitals (where an appalling 7 babies and 3 mothers died in just 8 months!). But that would mean taking time from praising themselves and each other for the purportedly “evidence based” care.
Instead, they are making fools of themselves on Twitter (again!) by trying to bully anyone who dares question their clinical judgment.
It started innocently enough when a British obstetrician tweeted me a link to this “empowering” story of an HBA3C attended by a British midwife.
I responded:
It’s like someone winning Russian Roulette and boasting that they were so smart to play.
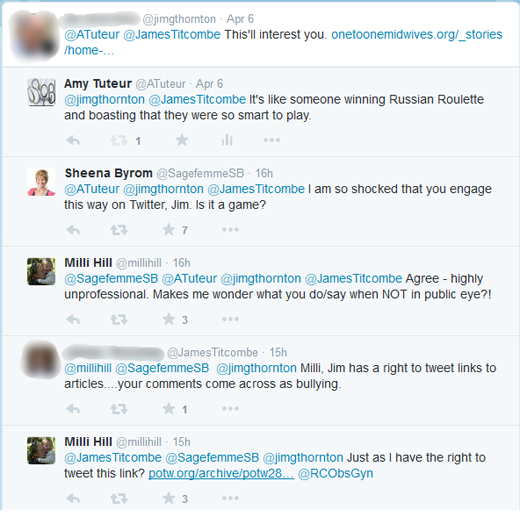
That’s when the midwifery bullies swept in.
Remember the cruel behavior of those mean girls from middle school and high school who appointed themselves arbiters of the social universe? It was never enough for them to exclude the girls they didn’t like. Nope, they set out to punish anyone who wouldn’t fall under their sway. The classic mean girl line? “You can’t be friends with me if you’re friends with her.”
Their hypocrisy is mind blowing, exceeded only by their stupidity in conducting their bullying in a public forum. What is wrong with these women?
Sheena Byrom, who has publicly treated a loss parent viciously, and who was not being addressed by the obstetrician, is “so shocked that you engage this way on Twitter.”
Pot, meet kettle!
And Milli Hill*, who wouldn’t know an obstetric fact if she fell over it, whines that it is “highly unprofessional,” and, as is apparently routine for UK natural childbirth bullies, sends the tweet to The Royal College of Obstetricians and Gynecologists. She also inanely links to a quote from MacBeth about the three witches, explaining that the combination of the obstetrician, the patient advocate and myself in one Tweet is just like them.

The thread twists and turns and branches off and I won’t bore you with the detaisl, but this is perhaps my favorite part:

The obstetrician tries to discuss the wisdom of a homebirth after 3 C-sections, but Milli Hill insists:
YOU should explain why you are tweeting with Amy Tutuer [sic]
There follows an flurry of midwives and natural childbirth advocates retweeting and favoriting each other’s tweets as if that might make them true.
The sad reality is that an obstetrician wants to discuss patient safety; the midwives and natural childbirth advocates want to bully anyone who tries to discuss patient safety. It is indicative of the UK natural childbirth culture and midwives, doulas and celebrity natural childbirth advocates who are out of control, specifically:
1. Patient safety appears to be irrelevant
2. Clinical guidelines are irrelevant
3. An obsession with “normal” birth regardless of the dangers
4. An inability to behave professionally online
5. A culture of bullying that spends more time on threatening dissenters than investigating (or even acknowledging) the deaths at their hands
6. A sense of invulnerability, as if they can say what they want, threaten whom they want, ignore what they want, and get away with it that extends from the highest to the lowest and, indeed, the bullying tactics are sanctioned by the highest and copied by the lowest.
Keep it up ladies, you’re doing a fabulous job at discrediting yourselves, far better than I could discredit you on my own!
*Addendum: Hill is deeply concerned that people might get the impression from this piece that she is a UK midwife when she is merely a celebrity midwifery apologist. Hopefully, this clears up any confusion.