
I’ve been writing for years that the World Health Organization conjured its “optimal” C-section rate of 10-15% from thin air. It is the childbirth lie that would not die. Now researchers from Harvard and Stanford have put a stake through its heart in the just published paper Relationship Between Cesarean Delivery Rate and Maternal and Neonatal Mortality.
More than 7 years ago I wrote:
[pullquote align=”right” color=”#4f933d”]There appears to be NO increased risk of either maternal or neonatal mortality for C-section rates as high as 55%.[/pullquote]
Anti-cesarean activists love to point out that the World Health Organization has recommended that the C-section rate should be 10-15%. Unfortunately, the WHO appears to have pulled those numbers out of thin air. Its own data shows that a 15% C-section rate does not result in the lowest possible levels of either neonatal mortality or maternal mortality…
At the time I compared international C-section rates with maternal and neonatal mortality rates and found:
The only countries with low rates of maternal and neonatal mortality have HIGH C-section rates … The average C-section rate for countries with low maternal and neonatal mortality is 22%, although rates as high as 36% are consistent with low rates of maternal and neonatal mortality.
Researchers from Harvard and Stanford just got around to performing the same calculations and this is what they found:
The optimal cesarean delivery rate in relation to maternal and neonatal mortality was approximately 19 cesarean deliveries per 100 live births.
In other words, they found almost exactly the same thing I found 7 years ago.
The graphs they created are quite impressive:
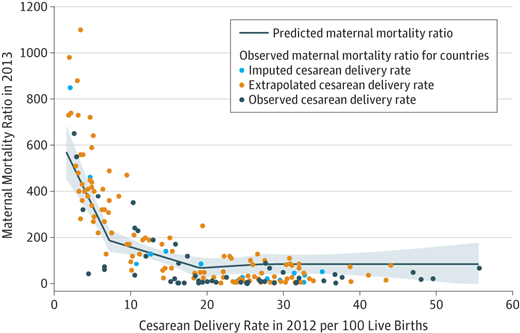
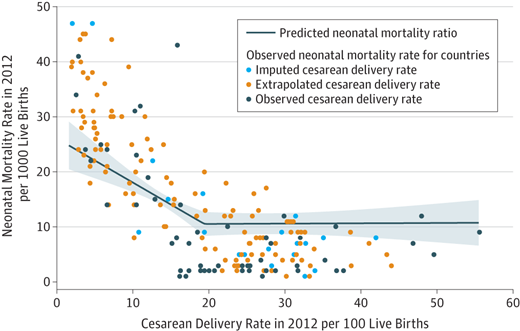
These graphs show that C-section rate below 19% lead to preventable maternal and neonatal deaths. In other words, they show that the WHO “optimal” rate, far from being optimal, is actually deadly.
They also show that C-section rates above 19% are NOT harmful. There appears to be NO increased risk of either maternal or neonatal mortality for rates as high as 55%.
According to the press release that accompanied the paper:
“On a nationwide level, our findings suggests there are many countries where not enough C-sections are being performed, meaning there is inadequate access to safe and timely emergency obstetrical care, and conversely, there are many countries where more C-sections are likely being performed than yield health benefits,” said Dr. Alex Haynes, primary investigator of the study, a surgeon and associate director of Ariadne Labs’ Safe Surgery Program. “This suggests on a policy level that benchmarks for C-section rates on country-wide level should be reexamined and could be higher than previously thought.”
But old prejudices die hard and journalists are already spinning the paper as an indictment of the US C-section rate. The Boston Globe insists Sky-high C-section rates in the US don’t translate to better birth outcomes. But they don’t translate to worse outcomes, either. Moreover, death is not the only outcome of concern. Many C-sections are done to prevent neonatal brain damage and to date there have been no international studies comparing C-section rates and rates of brain injury.
So it is entirely possible, indeed it is likely, that the optimal C-section rate is higher than 19%.
There are two main take home messages from the study.
The first is that C-section rates of less than 15% are UNSAFE. The WHO simply made up their optimal rate and basically ignored the scientific evidence. If I could figure out an optimal rate with some back of the napkin calculations 7 years ago, they could have figured it out, too. Their optimal rate reflected their personal prejudices, NOT science.
The second take home message has been obscured in the mindless demonization of C-sections that has been promoted by the natural childbirth industry: there is NO EVIDENCE of harm to mothers or babies from C-section rates as high as 55%.
The unreasoning prejudice against C-sections has got to stop. It’s not good for babies; it’s not good for mothers; and it’s not good for science.
This paper is a tiny first step.