
All posts by Amy Tuteur, MD
Kathy Dettwyler: formula-fed children definitely WILL BE INFERIOR

New motherhood is the last bastion of acceptable bullying and no one believes that more firmly than professional lactivists. Many are incensed by Courtney Jung’s book Lactivism, which shows definitively that the benefit of breastfeeding in industrialized countries has been dramatically overstated. In expressing their outrage they inadvertently demonstrate exactly the ugly, sanctimonious behavior that Jung decries.
Kathy Dettwyler, Associate Professor, Supplemental Faculty, Dept. of Anthropology, University of Delaware, Newark, is known for her cultural work on extended breastfeeding and weaning. What are her medical credentials? She has none, but that doesn’t stop her from pontificating on the benefits of breastmilk or bullying women for making feeding decisions of which she doesn’t approve.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Were you breastfed or bottle fed, Prof. Dettwyler. I’d like to know which is responsible for your viciousness.[/pullquote]
Responding to a heartfelt reader review of Lactivism on Amazon, Dettwlyer treats us to a glimpse of professional lactivism in all its malignant ugliness.
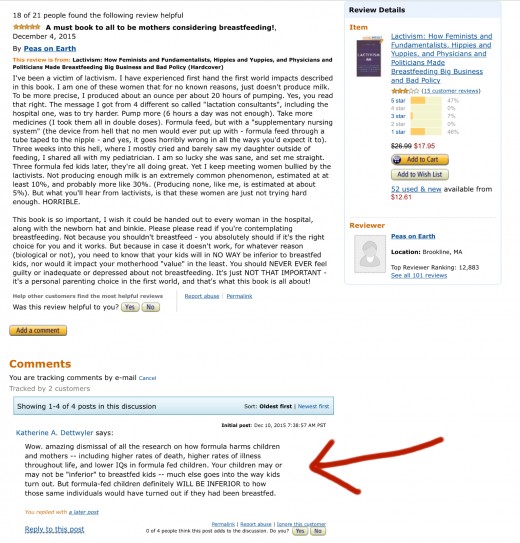
“Peas on Earth,” describes herself as a victim of lactivism. She is among the approximately 5% of women who CAN’T produce enough breastmilk to fully nourish an infant. She writes:
This book is so important, I wish it could be handed out to every woman in the hospital, along with the newborn hat and binkie. Please please read if you’re contemplating breastfeeding. Not because you shouldn’t breastfeed – you absolutely should if it’s the right choice for you and it works. But because in case it doesn’t work, for whatever reason (biological or not), you need to know that your kids will in NO WAY be inferior to breastfed kids, nor would it impact your motherhood “value” in the least. You should NEVER EVER feel guilty or inadequate or depressed about not breastfeeding. It’s just NOT THAT IMPORTANT – it’s a personal parenting choice in the first world, and that’s what this book is all about!
Who could disagree with that?
Kathy Dettwyler could and she publicly excoriates this poor woman:
… [F]ormula-fed children definitely WILL BE INFERIOR to how those same individuals would have turned out if they had been breastfed.
Really, Prof. Dettwyler?
Over the years I’ve read most of the major breastfeeding literature and I NEVER found even a single paper that demonstrated that formula fed children are inferior in any way to breastfed children. I’ve never read a paper from a reputable journal that even dared to advance that claim. Even those who invoke all sorts of unproven health benefits from breastfeeding haven’t thought to suggest that formula fed children are inferior. Even those who claim a tiny increase in IQ acknowledge out that this purported increase has no known impact in industrialized countries.
Here’s a thought, Prof. Dettwyler, how about taking a look at my Harvard yearbook and pointing out for us the formula fed graduates and explaining how much further they would have gone in life if only they had been breastfed? Wait, what? You can’t tell the difference between the formula fed and breastfed graduates? How can that be if formula leads to inferior human beings?
Or, better yet, how about making your ugly claims here on this blog and letting the physicians, scientists and statisticians who are regular readers school you on what the scientific literature actually shows instead of publicly berating a vulnerable mother on Amazon?
Wait, what? You don’t dare appear in any forum where others who know as much or more than you do could call you out for misrepresenting the scientific literature? You’re happy to publicly dish out viciousness but only in places where you can’t be held to account? Quelle surprise!
I’m sorry that Peas on Earth was subject to your viciousness, but I’m actually glad that you left your comment. You have illustrated the need for Jung’s book in a way that mere statistics never could.
I hope that you noticed my comment to you:

Were you breastfed of bottle fed, Ms. Dettwyler? I’d like to know which is responsible for your viciousness.
Lactivism and disciplining women’s bodies

With the possible exception of the author Courtney Jung, no one could be more thrilled about attention her book “Lactivism” is receiving than I am. The book has opened the door to the conversation that we need to have about the ways that natural parenting industries manipulate women into buying their products.
As everyone has undoubtedly heard by now, Lactivism rehearses the same arguments advanced by Joan Wolf in Is Breast Best? and Hanna Rosin in her Atlantic piece The Case Against Breast-feeding that the scientific evidence about the benefits of breastfeeding in industrialized countries is weak, conflicting and riddled with confounders. In fact, the only definitive benefits of breastfeeding are a few less colds and gastro-intestinal upsets across the population of infants in their first year.
[pullquote align=”right” color=”#F9B9D4″]Lactivism constricts the shape of mothering just as surely as the corset constricted the shape of women’s bodies.[/pullquote]
Lactivism has been reviewed by the NYTimes as a:
… riveting exposé of the forces that have turned the simple act of feeding one’s baby into a veritable battlefield, “to breast-feed or not to breast-feed” has become a question with far-reaching implications spanning medicine, politics, religion, feminism, commerce, race and social class.
Jung blames the lactation industry, including lactation consultants and breast pump manufacturers, for the moralization of breastfeeding. Indeed, as I have remarked in the past, the moralization of breastfeeding parallels the monetization of breastfeeding.
But there’s more going on here than merely an industry seeking profits. The unfortunate fact is that lactivism is just the New Age iteration of an age old tendency toward controlling women by disciplining their bodies. Lactivism, in conjunction with the philosophies of natural childbirth and attachment parenting, is the 21st Century equivalent of the corset. They constrict the shape of mothering just as surely as the corset constricts the shape of women’s bodies.
It is a sad fact of history that men have spent a tremendous amount of time policing women’s bodies. And an even sadder fact is that women have often been the prime enforcers in this effort. Natural childbirth was conjured by Grantly Dick-Read to convince white women of the “better” classes to drop efforts for political and economic equality and return home to have more children; La Leche League was created by a group of devout Catholic women who believed that mothers should not work outside the home and that convincing them to breastfeed was a way of keeping them there; and attachment parenting has been aggressively promoted by Bill and Martha Sears as “God’s plan” for ordering the family with the husband at its head and the wife as subservient.
The political, intellectual and economic emancipation of women that occurred in industrialized countries was one of the pivotal developments of the 20th Century. It brought with it tremendous social change, and tremendous social change rarely occurs without backlash. In my view, that backlash has been expressed on the political Right as the rise of religious fundamentalism that automatically relegates women to the home. It’s been expressed on the political Left as the rise of natural parenting (natural childbirth, lactivism, attachment parenting) that, though ostensibly about children and how they are raised, is really about women and what they are supposed to sacrifice when they have them. Lactivism, in company with natural childbirth and attachment parenting, renders women’s needs invisible, and when practiced with full adherence to its principles renders women invisible in the public sphere.
Jung is absolutely correct that lactivists grossly exaggerate the benefits of breastfeeding, and she is also correct that the moralization of breastfeeding has been promoted by the lactivism industry. In so doing, she has started a national conversation about whether a big business has promoted bad policy (it has!). But, in my judgment, that is just the beginning of the conversation we need to have. The real issue at stake is NOT how infants are fed; the real issue is how mothers of infants are supposed to behave in order to qualify for the designation “good mother.”
There is nothing wrong with breastfeeding or unmedicated childbirth or attachment parenting if those are the choices that work best for individual women and their families; I chose to do all of them with my own children. But there is something very wrong with philosophical movements devoted to forcing those choices on other women, essentially disciplining their bodies for every moment of the 9 months of pregnancy, the hours of labor and childbirth, and the years of parenting beyond.
It constricts the shape of mothering and while it may be big business, it is bad for women.
C-sections, asthma and white hat bias

The study of C-sections is afflicted with white hat bias.
What is white hat bias?
‘White hat bias’ [is] bias leading to distortion of information in the service of what may be perceived to be righteous ends… WHB bias may be conjectured to be fuelled by feelings of righteous zeal, indignation toward certain aspects of industry, or other factors. Readers should beware of WHB and … should seek methods to minimize it.
I’ve written about white hat bias before in relation to breastfeeding. In 2015 everyone “knows” that breast is best. Breastfeeding researchers are so sure that breastfeeding is beneficial that they exaggerate findings that place breastfeeding in a positive light.
[pullquote align=”right” color=””]It seems irresponsible to draw any conclusions from this data.[/pullquote]
Similarly, in 2015, everyone “knows” that the C-section rate is too high. Researchers are so sure that C-sections are harmful that they exaggerate findings that place C-sections in a negative light. A new paper about C-sections and asthma is a case in point.
According to yesterday’s New York Times:
For years, research has shown that babies born by cesarean section are more likely to develop health problems. Now, a groundbreaking study suggests that not all C-sections are equally risky…
Surprisingly, the data seemed to show more health problems among babies born by planned C-section than among those delivered by emergency C-section or vaginal birth, even though the planned surgery is done under more controlled conditions. The finding suggests that the arduous experience of labor — that exhausting, sweaty, utterly unpredictable yet often strangely exhilarating process — may give children a healthy start, even when it’s interrupted by a surgical birth.
Actually, the data on health problems caused by C-sections is weak and conflicting and this new study is more of the same.
The paper is Planned Cesarean Delivery at Term and Adverse Outcomes in Childhood Health by Akinbami et al. According to the authors:
Among offspring of women with first births in Scotland between 1993 and 2007, planned cesarean delivery compared with vaginal delivery (but not compared with unscheduled cesarean delivery) was associated with a small absolute increased risk of asthma requiring hospital admission, salbutamol inhaler prescription at age 5 years, and all-cause death by age 21 years. Further investigation is needed to understand whether the observed associations are causal.
What exactly did they find?
Compared with offspring born by unscheduled cesarean delivery (n = 56 015 [17.4%]), those born by planned cesarean delivery (12 355 [3.8%]) were at no significantly different risk of asthma requiring hospital admission, salbutamol inhaler prescription at age 5 years, obesity at age 5 years, inflammatory bowel disease, cancer, or death but were at increased risk of type 1 diabetes (0.66% vs 0.44%; difference, 0.22% [95% CI, 0.13%-0.31%]; adjusted hazard ratio [HR], 1.35 [95% CI, 1.05-1.75]). In comparison with children born vaginally (n = 252 917 [78.7%]), offspring born by planned cesarean delivery were at increased risk of asthma requiring hospital admission (3.73% vs 3.41%; difference, 0.32% [95% CI, 0.21%-0.42%]; adjusted HR, 1.22 [95% CI, 1.11-1.34]), salbutamol inhaler prescription at age 5 years (10.34% vs 9.62%; difference, 0.72% [95% CI, 0.36%-1.07%]; adjusted HR, 1.13 [95% CI, 1.01-1.26]), and death (0.40% vs 0.32%; difference, 0.08% [95% CI, 0.02%-1.00%]; adjusted HR, 1.41 [95% CI, 1.05-1.90]), whereas there were no significant differences in risk of obesity at age 5 years, inflammatory bowel disease, type 1 diabetes, or cancer.
Children born by planned C-section were at slightly increased risk of asthma requiring hospital admission, slightly increased risk of needing asthma medication at age 5 and increased risk of death both before age 1 and from 1-21. There were no significant differences in rates of obesity, inflammatory bowel disease, type I diabetes or cancer.

Comparing the effects of planned C-section to unplanned C-section revealed no difference in rates of asthma requiring hospital admission, need for asthma medication at age 5, obesity, inflammatory bowel disease, cancer or death, but an increased risk of type 1 diabetes.

So C-section appeared to slightly increase the risk of asthma (an auto-immune disease), but no other auto-immune diseases, and to increase the risk of unexplained death.
The authors also performed a sensitivity analysis. What is a sensitivity analysis?
The credibility or interpretation of the results of clinical trials relies on the validity of the methods of analysis or models used and their corresponding assumptions…
A sensitivity analysis addresses the validity of the assumptions used in calculating the results.
If, after performing sensitivity analyses the findings are consistent with those from the primary analysis and would lead to similar conclusions about treatment effect, the researcher is reassured that the underlying factor(s) had little or no influence or impact on the primary conclusions. In this situation, the results or the conclusions are said to be “robust”.
What was the result of the sensitivity analysis in this paper:
Complete case analyses comparing outcomes following planned cesarean delivery with unscheduled cesarean delivery demonstrated no significant differences in risk of any outcomes studied, as reported in Table 4. Complete-cases analysis revealed a significantly increased risk of offspring obesity at age 5 years following planned cesarean delivery compared with vaginal birth, but no significant differences in risk of salbutamol inhaler prescription at age 5 years, asthma requiring hospital admission, inflammatory bowel disease, cancer, or death up to age 21 years.
So, if I understand the sensitivity analysis correctly, it produced different results from the primary analysis, which means that the findings are NOT robust.
Nonetheless, the authors conclude:
Among offspring of women with first births in Scotland between 1993 and 2007, planned cesarean delivery compared with vaginal delivery (but not compared with unscheduled cesarean delivery) was associated with a small absolute increased risk of asthma requiring hospital admission, salbutamol inhaler prescription at age 5 years, and all-cause death by age 21 years. Further investigation is needed to understand whether the observed associations are causal.
It would have been more accurate to say that WEAK DATA showed a small absolute increase in the risk of asthma and unexplained death.
In other words, it seems rather irresponsible to draw any conclusions from this data. That didn’t stop the authors, though. They “know” that C-sections are bad and white hat bias led them to search until they found some weak data that seemed to support that pre-existing belief.
It’s yet another poor contribution to the confusing and conflicting papers that claim to show the “harms” of C-section, but, in truth, don’t show anything at all.
An excerpt from Push Back: Guilt in the Age of Natural Parenting
Last night I sent in the final edits for my forthcoming book Push Back: Guilt in the Age of Natural Parenting. I’m posting an excerpt in celebration. The book will be published by HarperCollins on April 5, 2016.
When I was a practicing obstetrician, I spent a lot of time correcting the misinformation of natural childbirth advocacy, and comforting women who had had healthy babies but still felt guilty for not “achieving” a vaginal birth or a birth without pain relief. Though I was aware of the emotional response from my bedside visits, it took years of blogging about the subject, corresponding with mothers, and arguing with activists to appreciate the true depth, breadth, and prevalence of misinformation coming from the natural parenting movement, and how this has come to blight the experience of mothering infants for so many.
Twenty years ago, when I began writing on the web, I thought that the problem could be solved with more and better information. Most of what passes for knowledge within natural childbirth, lactivist and natural parenting communities is flat out false. Yet simply correcting that myriad of falsehoods seemed to be fruitless. I came to understand that natural childbirth, lactivism and attachment parenting actually is about privileging the process over the outcome.
Natural childbirth, lactivism and attachment parenting are highly stylized, profoundly idealized representations of parenting. How do we know that they are idealized? Primarily it’s because the scientific evidence does not support most of their central tenets. That’s not to say that natural parenting advocates don’t believe in science; they do and they invoke science a lot. However, a close examination reveals that they often subvert the scientific evidence to arrive at predetermined conclusions.
Why would anyone want to subvert the scientific evidence on childbirth, breastfeeding and attachment parenting? Because each of these ideas have morphed into businesses, complete with trade unions, lobbying groups and brilliant marketing. Simply put, misinformation is being promoted by birth and breastfeeding professionals, as well as parenting gurus, as a way to make money. These factions portray doctors as the enemy, and their primary product has become distrust of the medical profession. They created alternate worlds of internal legitimacy in the same way that creationists and anti-vaccine activists had done before them, complete with books, journals, conferences and certifications to signify “expertise.” The internet has been their greatest enabler, allowing women to “research” parenting decisions without ever leaving a massive echo chamber.
There’s far more than money at stake. Beliefs about women and their role in society undergird natural parenting. It seems to me to be more than coincidence that natural childbirth, breastfeeding and natural parenting share a variety of disturbing characteristics: all imposed an inordinate amount of work and pain on women, and all ostensibly exclude fathers and other family members, making women not merely the primary caregivers but the only acceptable caregivers a majority of the time. And by requiring intense, round the clock effort, it makes it nearly impossible for women who want or need something in addition to mothering (a job, a career, free time) to be “good” mothers. It all seems suspiciously like the classic ploy to control and judge women by the performance of their reproductive organs.
When I dove deeper, I was not surprised to find that most of these movements were created or promulgated by elderly white men. Advocates represent natural childbirth, lactivism, and attachment parenting as the ultimate expressions of parental love, combining scientific evidence with maternal devotion, feminism and respect for maternal choice. The reality is far different. It is an interesting question how these philosophies that gather under the rubric of natural parenting put forward a pro-woman agenda but in fact are quite the opposite. In this book, I will show the evolution of each of the aspects of natural parenting—natural childbirth, lactivism and attachment parenting, from their origins to the big business they are today, from a search for authentic experiences to a prescribed experience that relegates women back into old-fashioned roles prescribed by gender.
Push Back tackles the natural parenting industry from all sides, hopefully alleviating guilt so many women unnecessarily face, revealing it to readers as the damaging, sometimes dangerous construct I think it is.
Midwives oppose the use of drugs in labor … unless they can administer them

Below are the characteristics of two types of pain relief in labor. Guess which one is favored by midwives.
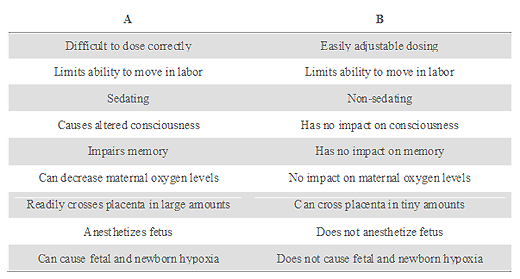
If you guessed “B,” you’d be wrong.
True, it is easily adjustable, non sedating, has no impact on memory or oxygen levels and crosses the placenta in miniscule amounts if at all. But it’s the dreaded epidural and it’s bad, bad, bad.
[pullquote align=”right” color=”#F87DD5″]All the pious wailing about the effects of epidurals are nothing more than hypocrisy. [/pullquote]
“A” is, in fact, favored by midwives and used extensively by midwives around the world at home and in the hospital. Indeed, many midwives believe it is perfectly compatible with natural childbirth despite the fact that it is most certainly a drug, marketed by a pharmaceutical company, is difficult to dose effectively, causes sedation and impaired memory, and readily crosses the placenta in large amounts where it sedates the baby.
Shocked? You shouldn’t be. Drug “A” is nitrous oxide and American midwives are clamoring for its use.
A new patient handout prepared by the Journal of Midwifery and Women’s Health expounds on the virtues of nitrous.
… Many women in Europe and other countries, such as Canada and Australia, use it to help cope with pain in labor. It is so common that in some countries as many as 8 in 10 women use nitrous oxide to help with labor pain. Women in these countries have been using this method of pain relief in labor safely for many years. Nitrous oxide hasn’t been used as often in the United States, but that is changing.
The handout acknowledges that nitrous produces altered consciousness and distorted memory, but apparently does not consider that a problem. The handout glosses over the impact of nitrous on the baby:
Nitrous oxide is the only pain relief method used for labor that is cleared from your body through your lungs. As soon as you pull the mask away, the effect of breathing the gas is gone within a few breaths. No extra monitoring is needed for you or the baby because you are using nitrous oxide. If you did get too sleepy, a monitor to check your oxygen levels might be placed on your finger. Nitrous oxide is safe for your baby, so if your baby’s heart rate is being checked intermittently (off and on) rather than continuously (all the time) with a fetal monitor, that is still okay…
Midwives are apparently unconcerned that nitrous crosses the placenta easily and in large amounts, producing sedation and altered consciousness in the baby. In fact, it would be quite accurate to state that nitrous “drugs” the baby whereas epidurals do not.
What’s the impact of nitrous on breastfeeding and newborn behavior? That’s not clear because very little research has been undertaken on the impact of nitrous on the newborn.
So by every parameter we can measure, nitrous has far more impact on women and babies than an epidural, yet nitrous is “good” and epidurals are “bad.” What accounts for this paradox?
It’s simple: midwives can administer nitrous, but lack the skills and training to administer epidurals.
All the pious wailing about the effects of epidurals are nothing more than hypocrisy. It really makes no difference to midwives whether women use “drugs” in labor to relieve pain, even if those drugs limit ability to move in labor, alter consciousness, impair memory, decrease oxygen levels, readily cross the placenta and sedate the fetus … just so long as they can administer the drugs.
This piece first appeared in December 2013.
UK trying to push women into homebirths that they don’t want

For many years, UK midwives and natural childbirth advocates insisted that a significant portion of women would choose homebirth if it were available to them. That hasn’t turned out to be the case. Despite increased promotion of and access to homebirth, despite research tailor made to promote the “safety” of homebirth, the UK homebirth rate has not increased very much at all.
But UK homebirth advocates haven’t given up. Their latest effort to force women into homebirths that they don’t want comes courtesy of NICE, the National Institute for Health and Clinical Excellence, who have decreed that pregnant women must be informed of interventions rates in all hospitals.
[pullquote align=”right” color=””]The promotion of homebirth rests on the belief that women’s agonizing pain in labor can be ignored.[/pullquote]
An article in The Daily Mail lays out the “problem”:
Statistically, home births or those in a small midwife-led unit are just as safe as hospital deliveries for women at low-risk of complications.
But most still choose to go to hospital, where doctors are immediately on-hand in case anything suddenly goes wrong.
Imagine that! Women want to give birth at the place best equipped to handle life threatening emergencies. We must discourage them from putting safety first!
The purported “solution”?
Guidance from NICE states that GPs or midwives should provide expectant mothers with information about the safety and risks of complication ‘specific to their local or neighbouring area’.
The information would state how many needed interventions such as forceps or caesareans, or suddenly needed to be transferred to hospital – if at home or in a midwife-led centre.
This may also include the numbers of stillbirths and women who died in labour – although these are likely to be very low.
Furthermore, these figures may not be accurately recorded as women who suddenly suffer a serious complication would be transferred.
The reason, of course, is to save money, though NICE denies it:
The watchdog insisted it wasn’t a cost cutting measure even though home births are far cheaper.
Figures show that a hospital delivery costs about £1,631, falling to £1,450 for a midwife centre and £1,066 for a home birth.
But hospitals are only cheaper when you don’t factor in pediatric costs for babies who are injured or die and when you ignore the fact that homebirth requires far higher levels of midwifery staffing than hospitals or birth centers do.
The real problem, though, is that the guidance is based on two very ugly premises. The first ugly premise is that birth without interventions is a worthy goal. It’s not; birth without DEATH OR INJURY should ALWAYS be the primary goal and the number of intervention is irrelevant. So called “normal birth” is a self-serving goal of midwives and they are trying to ram it down the throats of pregnant women. There is NO virtue to avoiding interventions merely to be able to say that you avoided interventions.
The second premise is even uglier and deeply misogynistic. The promotion of homebirth rests on the belief that women’s agonizing pain in labor can be ignored. I don’t notice anyone promoting home vasectomies or home transurethral prostatectomies even though the pain from those procedures is arguably less. What’s the difference? Men’s pain is always considered worthy of treatment whereas women are left to suffer, encouraged to suffer, and supposedly “improved” by suffering.
Effective pain relief is a human right, not just for men, but for women, too! The belief that women ought to endure pain or, worse, are improved by pain, is profoundly, irredeemably sexist in the extreme.
Homebirth is being forced on women because the government thinks it can save money and because the extremely powerful midwives union, the Royal College of Midwives, is more interested in promoting their autonomy and employment than promoting the comfort of women and the safety of babies.
And that is arguably the ugliest fact of all.
Stop obstetric violence toward babies, Janet Fraser!

You cannot make this stuff up
Janet Fraser, the Australian unassisted birth advocate who let her own baby die at homebirth has accused me of “obstetric violence.”
#endviolenceagainstwomen by Dr Amy Tuteur. Vicious vitriolic campaigning against women who experience #stillbirth #obstetric violence
You remember Janet, right? She’s the woman who, in the wake of her daughter’s entirely preventable death, declared:
[pullquote align=”right” color=”#fc0706″]There is such a thing as obstetric violence and it is perpetrated by homebirth advocates on babies.[/pullquote]
My birthrape with my first child is traumatic. My stillbirth was not.
As she went into the labor that eventually resulted in a dead baby, she actually gave an interview to an Australian newspaper on March 22,2009 in which she boasted of her decision:
Janet Fraser is in labour… Has she called the hospital to let them know what’s happening? “When you go on a skiing trip, do you call the hospital to say, ‘I’m coming down the mountain, can you set aside a spot for me in the emergency room?’ I don’t think so,” says Fraser, whose breathing sounds strained…
… She hasn’t seen a doctor or any health professional since becoming pregnant this time. No ultrasound, no genetic testing, no internal examinations, no stethoscope. Does she have any feeling for how long the labour will go? “I could do this for days. My daughter’s birth was 50-something hours. You just do it — it’s just birth, a normal physiological process.”
The baby was not born for another five days.
Fraser was excoriated by the coroner for her role in her baby’s death.
Essentially, Ms. Fraser was quite unprepared for what happened. There was not even a hard, flat surface available on which Roisin could be placed for resuscitation so these three amateurs – Ms. Fraser, Mr. Stokes and Ms. Duce, first placed the child on the rim of the inflatable pool and, when that proved unsatisfactory, used a chair. They were unable to abandon the chair and place Roisin on the floor in order effectively to administer CPR there because, the placenta not having been delivered, “that was as far as she would reach. ” Evidently, it occurred to nobody present to clamp and cut the cord and, anyway, Ms. Duce told the inquest, she had not been aware of the ready availability of any equipment to enable her to do so. According to Ms. Duce, further difficulties were encountered in administering CPR because Roisin was slippery and difhcult to hold and, evidently, it did not occur to anybody to wrap her in a towel although there were towels nearby.
And Fraser accuses me of obstetric violence?
There is such a thing as obstetric violence and it is perpetrated by homebirth advocates on babies.
Babies do not ask to be conceived. If a woman decides to conceive a baby and carry it to term, she has a moral obligation to care for the health and well being of that baby. She has a moral obligation to feed it and change it, and clothe it, and put it in a car seat when she takes the baby with her to the grocery store. She also has a moral obligation not to risk its life.
Obstetric violence toward babies involves real violence, injury and death, not hurt feelings. Over the years I have written about many women whose babies have died hideous deaths at homebirth.
These include breech babies whose heads were entrapped while their bodies dangled outside their mother’s vagina, and who died long before they could reach medical help.
They include babies who struggled for hours and suffocated, dropping dead into the hands of unsuspecting homebirth midwives who didn’t appropriately monitor their heart rates.
They include babies who slowly lost brain cells because their heads had delivered, but their shoulders became entrapped.
They include babies who died when they were suddenly extruded into their mother’s abdomen when a uterine incision ruptured and died for lack of oxygen long before they could reach a hospital.
They include babies who survived but suffered serious brain injuries leading to lifelong disabilities affecting their ability to move, to reason, to live on their own, to fulfill the potential that they had when labor started.
And, of course, they include babies like Roisin, whose mother’s hideous narcissism led to her death.
Who cares about the obstetric violence perpetrated on these babies?
Certainly not Janet Fraser who thinks everything is about her.
Certainly not homebirth midwives, who never met a risk they couldn’t label as a variation of normal.
Certainly not homebirth advocates, who never heard of a homebirth death that they couldn’t rationalize with the all purpose, and incredibly ugly claim that “some babies are just meant to die.”
As far as I’m concerned, there’s something very wrong when women claim that hurting their feelings is “violence. There is something very wrong when letting a baby suffocate to death, half the body born, and half still inside the mother is dismissed as inevitable, especially when it was not. And there is something very wrong when the obstetrician cares more about whether your baby lives or dies than you do.
As the Coroner noted at the inquest into Roisin Fraser’s death:
[Her views] are wrong views, extravagantly expressed and quite insensitive to the harm they may do to others, whether inexperienced mothers or children like Roisin whose chance of life was so unnecessarily put at risk. lf they seem intellectually valid or politically attractive to Ms. Fraser, she might give thought or more thought to the effect they may well have on children like Roisin.
Stop obstetric violence toward babies. Narcissism kills, as Janet Fraser continues to demonstrate.
Riddle: how many homebirth advocates does it take to change a light bulb?

Ten:
One to teach the course “Empower yourself by changing your own light bulb.”
One to whisper affirmations encouraging the light bulb to be in the correct position.
One to photograph the event.
One to tweet the event live.
One to fill the plastic kiddie pool. (Note: professional electricians claim that standing in water while changing a light bulb is dangerous, but they just say that to ruin your light bulb changing experience.)
One to call 911 if you get electrocuted while standing in water while changing the light bulb.
One to reassure you that people get electrocuted changing light bulbs even when they are not standing in water, so you shouldn’t let the warnings of those stupid electricians scare you.
One to help you eat while changing the light bulb in order to keep up your strength.
One to tell you to turn the bulb only when you get the urge.
And finally, one to actually change the light bulb and pretend to have an orgasm while doing it.
This piece first appeared in April 2010.
Nicola’s noxious narcissism: when the birth is more important than the baby

Which came first, the narcissism or the birth?
Damned if I know.
Regardless, something is very, very wrong when the birth is more important than the baby.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]We rolled the dice thinking it wouldn’t happen to us and we lost.[/pullquote]
Take Nicola for example.
After being “disrespected” during her first birth:
For my second pregnancy I chose to sit outside the system and hired independent midwives. I chose to birth at home against consultant advice as I didn’t trust them to look after my best interests. I put in a lot of work and effort to prepare myself for a natural birth which payed off as I had a wonderful birth.
Her work and effort paid off in a “wonderful” birth.
The birth was not wonderful for the baby, though.

But i was very unlucky, my baby was born not breathing 40 minutes away from hospital from which he has sustained serious brain injury and will live with serious life long disabilities.
Now I will spend the rest of my life wondering whether I should have gone against every instinct in my body and done as I was told by people I didn’t trust. If I had done that would my son have arrived safely??
Unlucky? Does Nicola blame herself for her son’s brain damage? Be serious!
…And it is likely he would have had a better outcome if he’d been born in the hospital, if I’d been hooked up to cfm. What a shame that my trust had been completely abused and destroyed first time round.”
And:
Birth is inherently risky. We rolled the dice thinking it wouldn’t happen to us and we lost.
Let me fix that for you Nicola. YOU rolled the dice with HIS life and HE lost.
It’s not a shame; it’s a tragedy that Nicola thought whether or not she was “disrespected” was more important than whether or not her son survived birth intact.
When exactly did the birth become more important than the baby?
Maybe Chrissy could tell us.
Here’s what she posted to her Facebook VBAC group:

I GOT MY VBAC!!!!! I want to share my vbac birth story with everyone.
What about the baby? You remember the baby, right? Ostensibly the entire purpose of the pregnancy?
Her was born at 28 weeks with intrauterine growth restriction, is intubated, in the NICU and potentially may not survive, but Chrissy knows what’s important to her. She GOT HER VBAC!!!!!
Carmina, on the other hand, seems stunned by what happened at her homebirth. According to the GoFundMe page:
T. was born on Wednesday, December 2, 2015 at home by mid wife. At some point during his birth two things went drastically wrong. He inhaled meconium which filled his lungs and the umbilical cord wrapped around his neck, cutting off his oxygen.
The midwife was able to rescusitate him after approximately 13 minutes, however, it is unknown how long T. had been cut off from oxygen intake, or at which point he inhaled the meconium. For the first 40 minutes of his life, he was not in Doctors’ hands as he was in route via helicopter to the Hospital.

According to his mother:
He was born at home, naturally with our amazing midwife … My water broke when his head came out and meconium spilled out … His umbilical cord was wrapped around his neck and I pushed his body out we could see he was blue and not breathing.
Our midwife immediately unwrapped the cord and started CPR. We called 911 and the ambulance got there in about 15-20 minutes … By the time I got to the hospital in an ambulance right behind him, they had him completely surrounded with a team of 8-10 …
The baby was transferred to another hospital:
Our plan was to wait until the next day … But then we received a phone called from the doctor that sounded very grim … We went to see T. and the doctor gave an update of how they cleaned him out as best they could and they were worried he had severe brain damage.
He underwent brain cooling therapy and at this point his prognosis was unknown.
It didn’t have to happen this way. Had his mother been more concerned about his safety than her experience, he’d be fine and she’d probably be complaining about her “unnecessary” C-section.
When did the birth experience become more important than the baby?
Maybe one of these women could explain it to us. Inquiring minds want to know.