People who venerate the natural imagine that this is nature.
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]The cute baby zebra is perfectly designed to be lunch for lions.[/pullquote]
It’s a cute little baby zebra, galloping with the herd. It’s perfectly designed to keep up with it’s mother. Born from her body, it was perfectly designed to stand within an hour of birth. It’s nourished by its mother’s milk, perfectly designed to meet its nutritional needs. But that’s a blinkered picture of nature, literally. Indeed, it was cropped from this image. Note the lion on the attack.

Because the sad truth about the cute baby zebra is it’s perfectly designed to be lunch for lions, and that’s what happened to it.

Advocates of natural parenting, natural eating and natural healing wax rhapsodic about the perfection of nature. But that’s because they imagine that the blinkered view they prefer is reality when it is nothing more than a comforting fantasy.
Focusing on the individual animal (or human) leads them to make statements like, “women are perfectly designed to give birth,” “breastmilk is the perfect food for babies” and “natural immunity is the best way to protect ourselves from diseases.” In contrast, if you zoom out to encompass the entirety of nature, it is obvious that nature doesn’t create perfection; it leads to the survival of only the fittest.
Zebras aren’t perfectly designed to survive until adulthood. By some estimates, as few as 27% of baby zebras survive their first year. Only the fittest — fastest, quickest to bolt, strongest — survive. What makes some baby zebras fitter than others? It’s genetics, their’s, their mothers’ and their herds’. Genetics makes some baby zebras faster than others. Genetics allows some zebra mothers to produce more milk than others. Genetics makes some herds collectively better adapted to their environment than others.
Remember the old joke: “How fast do you need to be to avoid getting eaten by a lion?” The answer: “Faster than the other guy!”
The same thing applies to baby zebras. The 27% of baby zebras who survive don’t do so because they are perfectly designed but merely because they are fitter —faster, quicker and stronger — than the 73% of baby zebras who didn’t make it.
Evolution isn’t merely acting on zebras, either. It is acting on all of nature including lions, for whom zebras are ideal prey. Evolution favors lions who are the fastest, quickest and strongest on the plain, and every increase in lion fitness comes at the expense of zebra survival.
If you look at the baby zebra in isolation, you might be fooled into thinking it is perfect. When you pull back to the wide angle view you can see that most baby zebras aren’t even “good enough” to survive, let alone perfect.
Similarly, women aren’t “perfectly designed” to give birth. In fact there’s a mismatch between what is perfect for the baby (to be born as late as possible with the largest brain size as possible) and what is perfect for women (to give birth as early as possible to the smallest size baby as possible). Evolution doesn’t ensure that all babies and all mothers will survive childbirth. A significant proportion will die and only the fittest survive childbirth. And just because they were fittest for childbirth doesn’t mean they are fittest for life outside the womb.
Modern obstetrics has changed that. Since surviving childbirth is entirely independent of surviving childhood, adulthood and old age, it only makes sense to employ childbirth interventions to save babies and mothers who would otherwise die. If you look at an uncomplicated vaginal birth in isolation, you — like natural childbirth advocates — might be fooled into thinking that childbirth is perfect. When you pull back to the wide angle view, the view that shows you the millions of children and mothers who routinely died in childbirth, you can see that childbirth is hardly an example of natural perfection.
Women aren’t “perfectly designed” to breastfeed. A substantial proportion of them aren’t capable of producing enough breastmilk, not because of “lack of support” but because of genetics. Babies aren’t perfectly designed to nurse at the breast, either. A significant proportion don’t have enough strength or muscle tone to extract what they need from the breast. In nature, they die. Today their mothers can pump breastmilk for them or give them formula. If you looked at a single baby who successfully nursed into toddlerhood you — like lactivists — might be fooled into thinking that breastfeeding is perfect. When you pull back to the wide angle view, the view that shows you the astronomically high infant mortality rate in nature, you can see that breastfeeding is hardly an example of natural perfection.
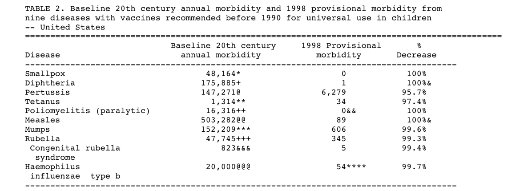
The same thing applies to vaccine preventable diseases. If you look at unvaccinated adults who survived childhood diseases unscathed you — like anti-vaxxers — might be fooled into thinking that natural immunity is all that we need. When you pull back to the wide angle view, the view of cemeteries filled with children and adults who routinely died from vaccine preventable diseases, it makes it crystal clear that natural immunity is far inferior to vaccine induced immunity.
Natural childbirth advocates, lactivists and anti-vaxxers have a profoundly blinkered view of nature. Imagining that natural childbirth, breastfeeding and natural immunity are perfect is no different from imagining that all baby zebras are designed to survive lion attacks … and just as foolish.