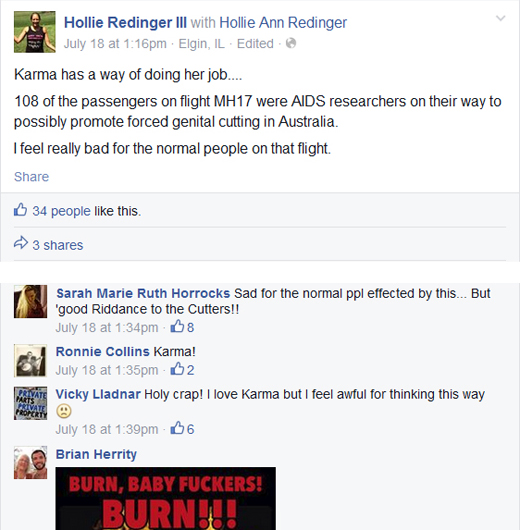
Apparently foreskins are more important than people.
From the Facebook page of intactivist (and anti-vax activist) Hollie Redinger.
For once I am speechless.
Apparently foreskins are more important than people.
From the Facebook page of intactivist (and anti-vax activist) Hollie Redinger.
For once I am speechless.

Is Milli Hill deliberately lying or just ignorant?
Consider the way she begins her latest piece Is childbirth really such a ‘risky’ business?:
If you believe everything you read, then you probably think that childbirth is one of the riskiest activities any human can undertake.
Actually, it isn’t, and statistically you’re massively more likely to meet your maker behind the wheel of your motor.
Ummm, Milli, here’s a newsflash: childbirth IS one of the riskiest activities any human can undertake and you or your baby are MUCH more likely to die in childbirth than in an automobile accident.
Childbirth is and has always been, in every time, place and culture, a leading cause of death of young women and THE leading cause of death of babies. Indeed, according to Save the Children, the day of birth in the most dangerous day of the 18 years of childhood.
Childbirth seems safe only because of modern obstetrics. Obstetrics has lowered the perinatal mortality rate 90% and the maternal mortality rate 99% in the past 100 years. But midwives cannot provide many of the services that have made childbirth so safe and therefore, for their own economic self interest, they and their apologists like Hill deny that those safety measures are really necessary.
Homebirth and natural childbirth advocates keep throwing memes against the wall, hoping one will stick. Obstetricians don’t follow scientific evidence! Except that they do. The media is to blame for the pain of childbirth! Except that it isn’t. Homebirth is a human right! Except that it’s not. A healthy baby isn’t enough! Except that for most women, it is. The latest entry in the midwifery meme collection is childbirth isn’t risky!
Except that it is.
Consider what Cathy Warwick, head of the Royal College of Midwives has to say on the subject:
There is concern at the RCM and among midwives, that our focus on risk, and the way that we are describing risk, is making women feel scared. Ironically, creating fear, in itself, causes risk – if women are fearful then they are less likely to release the hormones needed for a straightforward birth.
Does Warwick actually believe the nonsense that comes out of her mouth?
She’s already been forced to publicly retract one of her completely fabricated claims. Warwick claimed that the Netherlands, which has a high rate of homebirth, the lowest perinatal mortality levels for babies in Europe. Just one problem: The Netherlands has one of the HIGHEST perinatal mortality rates in Western Europe. Oops!
Now, she’s spewing nonsense about risk. Ms. Warwick’s behavior is especially disturbing given the sad state of midwifery in the UK. After a spate of preventable perinatal and maternal deaths due to midwives being unwilling to call other specialists; after a government report that revealed that 20% of obstetric funding now goes for liability; and after another government report that chastised midwives for covering up the deaths at the hands of their colleagues, one might think that Ms. Warwick would be busy doing whatever she could to promote better outcomes. Instead, she seems to think her job is to promote employment opportunities for midwives.
Lying about, dismissing or discounting the risks of childbirth is deeply unethical. We would rightfully be shocked by a physician who represented heart surgery as without risk or even plastic surgery as without risk. Women need to know the REAL risks and benefits, both of procedures AND of refusing procedures. We should be equally shocked by midwives like Warwick (and her cheerleaders like Hill) who represent childbirth as without risk, or refer to the “risks” of childbirth in scare quotes.
No one should forget that midwifery is a business, and it is part of the larger industry of natural childbirth. Both earn profits by convincing women to forgo interventions, pain relief and safety measures. Emotional manipulation of women is key to the success of the industry, and the emotional manipulation includes chivvying women into rejecting safety measures by being fundamentally dishonest about the very real dangers of childbirth.
Warwick and her cheerleader Ms. Hill should be embarrassed by their defense of the status quo and by the fact that they are either actively misrepresenting the risks of childbirth or simply ignorant of them. Either way, they are failing in their ethical obligation to be honest about the risks of birth and serving an industry (the natural childbirth industry) that profits by being dishonest about those risks.

What would the world of homebirth look like if it were nothing more than middle school writ large?
It would look an awful lot like the world of homebirth looks today. Homebirth, like middle school is dominated by Queen Bees, based on exhibitionism and risky behavior, and ruled through enforced conformity, emotional manipulation, shunning, and purging.
The world of homebirth is dominated by Queen Bees. You know the type. They only feel alive when they are controlling a group of sycophants; hence they have blogs and websites restricted to sycophants. They run the gamut from complete wackos like Ina May Gaskin, Gloria Lemay, and Janet Fraser to mainstream business people like Jen Kamel, Gina Crosly-Corcoran, and Ricki Lake, to know nothings like Carla Hartley and January Harshe.
They are characterized by narcissism and overweening arrogance. They don’t need no stinkin’ medical or midwifery training to appoint themselves as experts on childbirth. They know what’s best for you in every situation, even though they don’t know you at all. What’s best for you is to copy them, to worship them at their seminars and workshops, and to buy their goods and services.
They demand rigid conformity to arbitrary rules:
You must not have a C-section or you must be devastated if you do. You must not have pain relief in labor or you must be ashamed if you do. High risk pregnancy? Your fault. Breastfeeding painful? Your fault. Baby died at homebirth? Bad stuff happens.
It’s is always your fault, except when it happens to them. When Queen Bees fail to meet their own arbitrary rules it’s the hospital’s fault: They had to get the epidural because the nurse mentioned it, or their heplock was too painful. Their C-sections were foisted on them by their doctors, even the C-sections they asked for. Their own complications never would have happened if they had had an unhindered labor.
Exhibitionism is key. You must demonstrate your conformity by filming your baby’s birth and posting it on YouTube for the world to evaluate. You must post your birth story in contraction by contraction detail so the Queen Bees of the homebirth world can parse it for ideological correctness. The more risky your exhibitionism is, the better. Breech baby? Twins? VBA4C? Awesome! The greater the risk of death, the more evidence that you are loyal to the Queen Bees’ arbitrary rules, and the higher your status in the group.
What if you refuse to conform? What if you don’t feel bad that you deviated from the Queen Bee’s rules? What if, horror of horrors, you don’t constantly feed the Queen Bee’s insatiable need for praise and worship. In those cases, Queen Bees have ways of dealing with you.
The first step is emotional manipulation through shaming. You are weak. You are selfish. You are a BAD MOTHER!
So long as you recognize the error of your ways, come slinking back promising to do better next time, and praising the Queen Bee for achieving what you could not achieve, you are allowed to remain in the group.
And if you don’t? You must be purged from the group and shunned. No one is to speak with you or acknowledge you. Whatever you write is greeted with the metaphorical equivalent of the Queen Bee putting her fingers in her ears and chanting “la, la, la, la, la.”
Why? Because, according to the Queen Bee, you are mean to her, bullying her, a troll and, horror of horrors, not supportive. That’s because the Queen Bee lives in a Manichean world where you are either with her or against her. There is no middle ground. She claims that she is protecting her group from unsupportive comments, but, really, she is protecting her fragile ego from anyone who doesn’t acknowledge her as the Queen.
This middle school behavior has important implications for a woman considering homebirth.
She needs to ask herself whether she is choosing homebirth because it is right for her and her baby or because it cements membership in the Queen Bee’s circle. That goes double for those planning a high risk homebirths where the possibility of her baby’s deaths is much higher.
She need to ask herself whether the “encouragement” she is getting for her planned homebirth is truly encouragement or just a way to bolster the Queen Bee’s fragile ego by having her own choices mirrored back to her.
When she is shunned for questioning the arbitrary rules of the Queen Bee, she needs to ask herself why the Queen Bee’s approval is so important to her.
When she is shamed for daring to deviate from the Queen Bee’s prescriptions for birth, she should recognize that the Queen Bee and her sycophants are not her friends. Friends help you when you are down. They don’t crush you.
When she is purged from the group for not being sufficiently worshipful of the Queen Bee, she should thank her lucky stars for being forced out of a toxic situation.
And in the worse case scenario, when her baby dies because she attempted a homebirth, she should never look to the Queen Bee for accountability. Indeed, she should prepare herself to be vilified by her former community; her empty arms and broken hear will be a source of unbearable cognitive dissonance to the Queen Bee and her sycophants.
The world of homebirth isn’t about babies and it isn’t about birth. It’s about Queen Bees enforcing their will through ideological conformity, emotional manipulation and shunning of those who deviate … just like middle school.

A guest post from a registered nurse (RN):
I used to be an assistant to a lay midwife who delivered babies in her own home. I was so ignorant, and I didn’t KNOW I was ignorant! The midwife didn’t recognize her ignorance either.
I really had no idea of the difference in education between CNM, CPM, and DEM. This particular midwife is completely self-taught, a “granny” midwife with no medical background. When I was assisting her, she delivered approx. 200 babies a year. She did not have OB back-up, but she did have a certain amount of respect from the local doctors and hospital, who accepted her transfers without hassle. That respect was probably because she at least didn’t try to do vaginal births at all cost and she did not wait too long to transfer. Also some respect simply because of her persona. She makes you feel like she is in charge, and just knows things. I’ve heard local medical personnel make remarks like “K really has a knack and intuition for midwifery, doesn’t she?” This persona is what makes the mothers feel safe with her. At first I thought she “knew” everything too. But as I worked with her, I began realizing that it wasn’t true. I tried to change how some things were done, but the lay midwife became upset. No one was allowed to threaten her little kingdom! So I left.
I became a registered nurse, and got a job working in a Labor and Delivery unit. Then I began to understand how little I really knew, and how deficient and downright dangerous the lay midwives are! As has been pointed out on your blog so often, when you are ignorant you don’t KNOW you are ignorant!
I used to believe what the midwife said, that the apprenticeship model is just as valid as formal education. She used to say “I would much rather have an experienced midwife (DEM) attend me than a CNM just out of school.” I, of course, thought that made complete sense. But that is complete BS, because you have no idea how the DEM practices or how accountable she is. The new CNM has real medical professionals looking over her shoulder until she has the necessary experience to practice safely.
This is why there should be uniform standards of education and practice for ALL midwives. The following paragraphs are very specific examples of direct entry midwifery practices as I experienced them.
She accepts anyone who wants to VBAC, regardless of the client’s history. I never heard her asking anyone what type of uterine incision she had. It wasn’t until I became an RN that I learned a woman should never TOLAC after a classical incision, I doubt she even knows that. Now I’m amazed that we never had a rupture that I know of (during the time I assisted her at least).
There’s no understanding of hemodynamics, and what acute blood loss can do to the body. What are signs of too much blood loss? Um, we didn’t know. We took one blood pressure after delivery and that was it. No pulse, no O2 sat. I didn’t know what a dangerously low blood pressure was until I was in nursing school. I knew how to take vital signs, but I had no idea how to interpret them. I didn’t know what they would look like when a woman was hemorrhaging. I don’t think the midwife knew either because she never took vital signs. So when did we transfer for hemorrhage? When the woman was lying in a pool of blood and passing out. Estimated blood loss? No idea. We estimated it in terms of a little, medium, a lot. No idea how many mLs. This is why it is easy for me to believe that the midwives in Australia didn’t recognize the signs of acute blood loss in Caroline Lovell’s case. Lay midwives are not trained professionals, they don’t know!!!
She didn’t know how to do perineal repairs. She always told the women to “keep their legs together for several weeks” and the lacerations would heal just fine. Once or twice I saw her put several random stitches in the perineum, but never any vaginal repair. She had no idea how to do it; therefore it would heal “just fine”. Not enough education!!
Prenatal visits consisted of a blood pressure check, FHT with doppler, manual palpation of fundal height and estimation (no actual measurement), and external position check. No weight check. Cervical exams were done close to term. A primip was sent to her PCP for a blood type to check RH. No other blood work was ever done, unless a mom specifically asked for it. Most moms were routinely given oral iron to cover any potential anemia, and they all got calcium and a prenatal vitamin. There were no urine checks for protein, no GBS testing, and no testing for gestational diabetes. No ultrasounds, unless the midwife had a question about position or the woman had a prior infant with an anomaly. Of course she had mostly low-risk women. They were “low-risk” because she didn’t check for any conditions that might make them high-risk, or really even know what conditions are high-risk. Not enough education!
So we didn’t have any gestational diabetics (because we didn’t test for it), of course we didn’t have to follow any newborn glucoses either. But of course, we had no idea that newborns might have a problem with their glucose because we had never learned about that!
She did no newborn exams, no newborn vital signs. She never laid a stethoscope on the newborns at all, nor checked their temperatures. And even if she had, she didn’t know normal parameters for newborn respiratory rates. Most babies got apgars of 9/10, some even 10/10. No babies got any eye prophylaxis or Vit K. There was no breastfeeding support offered.
There was no continuous fetal monitoring during labor, only doppler checks every once in a while. She did no charting at all, so there were no scheduled time intervals by which checks must be done, just when she happened to think about it. I had no idea about decels or fetal distress. I thought if you put a Doppler on the belly and the FHT are below 120, the baby is in distress. I didn’t know there was such a thing as late decels or what they meant. In second stage the baby was monitored once or twice. When we had a baby with low apgars, it was always “with no warning”, and “the baby was fine all through labor”.
She was not NRP certified nor was she even CPR certified. She carries oxygen and an infant bag with mask, and attempts resuscitation if needed. It impresses the parents, but isn’t much good actually. Now I have a NICU resuscitation team 30 seconds away from each delivery and I realize how inadequate our efforts were. Not enough training and education! Her assistants now are not required to have even CPR training and have no idea how newborn resuscitation is done.
She attempted external versions for breech and transverse lie. She delivered breech and twins. She had no idea of whether twins are di/di or not, nor any idea of the significance of that.
She used “black market” Pitocin for postpartum hemorrhages. But she didn’t stick to postpartum use. She gave it to augment stalled labor. How could she do that, without IV access? Simple, she gave it subcutaneously, in small amounts. And it worked. Now I’m appalled, aghast, at how recklessly dangerous that is without CEFM. I had no idea! Not enough education!!! There are many other OOH midwives doing the same thing.
She never used sterile gloves, or set up a sterile field for deliveries. Sterilization of instruments consisted of wiping them off with alcohol.
This midwife’s clientele is almost exclusively Amish. She practices near one of the largest Amish communities in the US in a state where lay midwives operate in a “gray area” legally. She likes it that way because the Amish women don’t question her, trust her implicitly, and will not pursue litigation or repercussions of any kind. They call her for any kind of medical questions they have, even outside of women’s health, and she freely dispenses medical advice over the phone without seeing the patient in question. Sometimes her advice even contradicts a doctor’s advice. . .guess whose opinion carries the most weight?
The only way to make homebirths safer is abolish the CPM and DEM, and require all midwives to be CNMs. I do think the Amish should be able to have an OOH birth option, as this is more compatible with their lifestyle. They are not doing homebirths to be crunchy or because they believe in vaginal births at all costs. They have never even heard of the “Business of being Born”. But they do deserve better care than they are getting. Every woman deserves professional medical care!!

I am humbled by the profound love that James Titcombe has shown for his son Joshua.
James and his wife Hoa lost their son to midwifery incompetence (Joshua’s easily preventable, tragic hospital birth death). According to an National Health Service investigation quoted by The Independent:
Joshua died in November 2008, nine days after being born at the Furness General Hospital, part of the University Hospitals of Morecambe Bay NHS Foundation Trust. An inquest in 2011 said that staff at the hospital failed to spot a common infection, and that he would have stood an 80 per cent chance of survival if antibiotics had been delivered in the hours after his delivery.
The pain and frustration that James Titcombe deals with must be immense. The NHS initially refused to investigate, but James continued to advocate for Joshua. When he decided to take a break from his years of pressing for an investigation, he was treated with unspeakable contempt. According to The Independent:
The family were left deeply hurt on two occasions after seeing internal email exchanges between Trust staff. One followed an email from Mr Titcombe in June 2010 saying he would be stepping back from his inquiries after “becoming extremely distressed and anxious” about the investigations progress.
Informing the Trust’s head of midwifery of the email, the Trust’s customer care manager wrote: ‘Good news to pass on re [Mr D]’, and received the reply: ‘Has [Mr D] moved to Thailand? What is the good news?’
In another email from August 2009, later seen by Mr Titcombe, a discussion of a midwife’s statement to the Nursing and Midwifery Council (NMC) concerning the circumstances of Joshua’s death was subject lined: “NMC shit”.
But James did not give up. He fought on for Joshua and ultimately he and Hoa received an apology from NHS for not investigating Joshua’s death back in 2010, and an apology for the inappropriate emails.
James has continue to advocate on behalf of other babies, so no parent will have to endure the preventable death of a baby, a refusal to investigate it, and the contemptuous treatment that followed it.
UK midwife Sheena Byrom and her colleagues are familiar with James’ efforts and apparently consider him ever so tiresome.
Byrom and colleagues were having a public Twitter confab on the use of social media during and after birth (just like nature intended, no doubt). Byrom tweeted that hospital policies appeared to be dictated by risk and “all this talk about risk. Not comfortable with it.”
James entered the Twitter stream to point out that childbirth is indeed quite dangerous. He should know. His son died as a result of an infection acquired during birth.
A chilling response from Byrom and colleagues follows:

Highlights include:
oh James-don’t let’s get on that roll again …
and:
getting out of bed in the morning has risks http://homebirth.org.nz/magazine/article/climbing-trees/
Yes, James, how could you be so tiresome, always going on about the risks of childbirth and the babies who die as a result? Sheena is so over that.
Sheena ought to be ashamed of herself for the chilling way that she dismissed the father of a baby who died as a result of midwifery incompetence. But that would involve insight, compassion and a sense of responsibility, something in woefully short supply among UK midwives.
How can women trust “professionals” who dismiss a dead baby as a troublesome distraction from the agenda of promoting midwifery?
And how can women trust “professionals” who are aggressively close minded. When I posted a link to my piece debunking the article that Sheena cited, she responded thus:
don’t read your foolish, dangerous blogs, you are blocked.
and:

It’s almost as if Sheena and colleagues fear that by reading my blog, they might learn something they did not want to know. And that could be “toxic and dangerous” to them (who cares about babies and women who might be saved?).
Byrom’s contemptuous dismissal of James Titcombe, a father whose son died of midwifery incompetence, who was forced to endure a refusal to investigate his son’s death, and subject to chilling emails that treated his dead son as an inconvenience, is both outrageous and disgusting.
Her refusal to read my blog is indicative of the close mindedness of UK midwives who prize validation above scientific evidence, process above outcomes, and midwifery income above the lives of babies and mothers.
Sheena Byrom, have you no shame?
Oh, wait, you’re a UK midwifery leader, so of course you don’t.


When my husband and I were first married, we didn’t have much money, and, therefore, didn’t have a lot of choices in housing. Our apartment, while conveniently located, had certain problems including a cockroach infestation. Every morning when we turned on the light in the windowless kitchen, dozens of cockroaches would scurry out of the light back into the darkness.
I hadn’t thought about that daily occurrence in many years until it recently came to me that birth bloggers are like cockroaches. They, too, gather in the darkness and scurry away when the light of science is shined upon them. That’s because they KNOW that they cannot defend their claims against actual scientific evidence.
Unlike cockroaches, however, birth bloggers can turn off the light when they are exposed. How?
1. The natural habitat of the birth blogger is her own blog, where she decides how much light, if any, is shed on actual scientific evidence.
2. Birth bloggers almost never stray outside their blogs because they will be crushed in the light of scientific evidence. Hence, they never attend mainstream conferences, they never speak at medical conferences, are never invited to sit on expert panels, are never invited to testify in malpractice cases, and are not considered “experts” by anyone but themselves.
3. Birth bloggers invite visitors to their natural habitats, but protect themselves from the light of scientific evidence by deleting and banning any commentors who dare to question them or to present evidence that they chose to ignore.
4. Birth bloggers thrive in the darkness of ignorance and gullibility of their readers. Anyone with actual scientific knowledge would laugh at them.
5. Birth bloggers, like cockroaches have highly evolved defense mechanisms. Birth bloggers are evidence-resistant. They start from a conclusion and work back to cherry pick evidence to support it, while ignoring the larger body of evidence that debunks their conclusions.
6. Birth bloggers find support in numbers. They proliferate like cockroaches and no sooner is one crushed by the weight of scientific evidence, then another repeats the same lies that the first couldn’t rebut.
When we shined the light of science on the hideous rupture rate in Jen Kamel’s VBACFacts group, she ruthlessly purged the group, leaving her followers in the dark about the truth. When we shine the light of science on Rebecca Dekker’s assertion that her claims are “evidence based,” she deletes them and bans commentors, leaving her followers in the dark about the truth. The Lamaze blog Science and Sensibility routinely vets comments to be sure that their followers are left in the dark about real scientific evidence. Indeed, there is not a birth blogger that I am aware of who doesn’t routinely ban and delete when presented with scientific evidence.
Why are these birth bloggers afraid of the light? Because, like cockroaches, they know they will be easily crushed when people can see them for who they are: lay people who promote and profit from pseudoscientific nonsense.
How can women protect themselves from the infestation of birth bloggers? It’s pretty simple.
Never trust the information you get from a birth website that heavily moderates, deletes and bans. It means that, just like cockroaches, they are hiding in the dark. They wouldn’t need to heavily moderate, delete and ban if what they are write were true.
One of the favorite memes of advocates is that natural childbirth is “evidence based,” while obstetricians ignore scientific evidence. Childbirth blog, websites and message boards slap “evidence based” over whatever nonsense they dream up, and figure that the gullible public will look no further.
A good rule of thumb for anyone researching childbirth is this: if a natural childbirth website calls itself “evidence based,” it almost certainly purveying pseudoscience dressed up as science. The website of cardiology nurse Rebecca Dekker, Evidence Based Birth is a prime example. As the saying goes, you can put lipstick on a pig, but it’s still a pig, and in the world of childbirth, “Evidence Based Birth” is a big fat pig covered with lots of lipstick.*
How can you tell the difference between science and pseudoscience dressed up as science? This image from I fucking love science lays out the general principles.
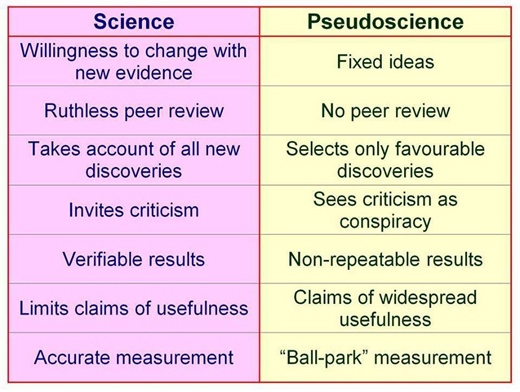
The primary difference between science and pseudoscience is a willingness to change based on new evidence. Pseudoscience, in contrast, starts with a conclusion and defends it regardless of the evidence.
Rebecca Dekker starts with the premise that the tenets of natural childbirth are true and looks for evidence that confirms those tenets. She ignores evidence that does not support natural childbirth, and is not above deliberately misleading readers by posing one question, but answering another.
Her recent piece on waterbirth, Evidence on the Safety of Water Birth, is a classic in this genre. Dekker starts with the premise that waterbirth is safe and cherry picks evidence to support that claim while ignoring or inappropriately dismissing evidence that shows the opposite.
What is waterbirth? It is the practice of giving birth a plastic pool of water that is inevitably fecally contaminated. It is the equivalent of giving birth in a toilet, and has similar risks, including the risk that the baby will breathe in or swallow the fecally contaminated water.
The American Academy of Pediatrics’ Committee on Fetus and Newborn in conjunction with the American College of Obstetricians and Gynecologists has recently updated its position on waterbirth. Nothing has changed since the previous edition published in 2005, except in the intervening years more cases of perinatal death and injury have been reported.
Some of the reported concerns include higher risk of maternal and neonatal infections, particularly with ruptured membranes; difficulties in neonatal thermoregulation; umbilical cord avulsion and umbilical cord rupture while the newborn infant is lifted or maneuvered through and from the underwater pool at delivery, which leads to serious hemorrhage and shock; respiratory distress and hyponatremia that results from tub-water aspiration (drowning or near drowning); and seizures and perinatal asphyxia. (my emphasis)
But, hey, that’s just the way that the American Academy of Pediatrics’ Committee on Fetus and Newborn and the American College of Obstetricians and Gynecologists assess the scientific literature. Cardiology nurse Rebecca Dekker thinks she knows better.
Her piece contains lots and lots and lots of words, but her conclusion is pretty simple. The evidence that currently exists is less than the highest quality evidence.
Duh!
The AAP and ACOG are well aware of that. They are invoking the precautionary principle. What’s the precautionary principle?
According to Wikipedia:
The precautionary principle … states that if an action or policy has a suspected risk of causing harm to the public or to the environment, in the absence of scientific consensus that the action or policy is not harmful, the burden of proof that it is not harmful falls on those taking an action.
In other words, in the absence of high quality evidence that waterbirth is safe, it should not be standard care. AND it is up to the proponents of waterbirth to provide that high quality evidence before waterbirth can be recommended.
But Dekker completely ignores the precautionary principle in her conclusion.
According to Dekker:
Based on the data that we have, waterbirth is a reasonable option for low-risk women during childbirth, provided that they understand the potential benefits and risks. If women have a strong desire for waterbirth, and there are experienced care providers who are comfortable in attending waterbirths, then at this time there is no evidence to deny women this option of pain relief.
Simply put, the AAP and ACOG believes (in conjunction with Dekker) that there is no high quality evidence to support waterbirth, and a growing body of lower quality evidence that waterbirth kills babies who breathe in the fecally contaminated water or swallow it during birth. Dekker starts with the conclusion that waterbirth must be safe, dismisses the existing evidence on the deaths that resulted from waterbirth, and asserts that it must be considered safe until it is definitely proven to be deadly. Dekker’s claim about the safety of waterbirth isn’t evidence based; it’s her opinion.
The same thing goes for nearly everything on her site. That is presumably why Dekker isn’t spending any time speaking in any venue where she could educate pediatricians or obstetricians about their purported errors in evidence interpretation. She knows she’d be laughed off the stage. She isn’t writing for physicians or scientists, either, because they would eviscerate her claims in short order. She writes for lay people who aren’t capable of assessing the validity of her claims and, in many cases are merely looking for justification to ignore the advice of pediatricians and obstetricians.
A more accurate moniker for her website would be “Rebecca Dekker’s Opinion on Birth,” but who is going to take that seriously? Instead, she calls it “Evidence Based Birth.” Dekker can put lipstick on a pig of a website, but it’s still a pig.
*Dekker basically admits this in her website disclaimer:
The information presented here does not substitute for a healthcare provider-patient relationship nor does it constitute medical advice of any kind… The opinions expressed in this blog are strictly the author’s personal opinions … The information on this blog may be changed without notice and is not guaranteed to be complete, correct, timely, current, or up-to-date…(my emphasis)

Ideological consistency has never been a hallmark of the natural childbirth movement, (childbirth is painful/no, it’s orgasmic; I didn’t need any pain relief/I couldn’t have done it without the birth pool; I am a warrior birth goddess who can withstand any amount of pain/I can’t bear to have a heplock), but it often seems that the inconsistency reaches its apogee around the issue of C-sections.
The phrase “too posh to push” suggests that choosing a C-section (for breech, after a previous C-section, without a medical indication) is the easy way. It implies that women who choose C-sections are lazy and can’t be bothered with the hard work of pushing a baby out through the vagina.
Yet ask a natural childbirth advocates why she fears a C-section and will go to extraordinary lengths to avoid one, and she’ll tell you that it is because C-sections are so painful, and the recovery is so long and difficult that it compromises the ability to bond to and care for a newborn.
So which is it? Are C-sections easy or are they hard.
Lactivists seem to have a similar problem with the issue of breastfeeding. They can’t seem to decide whether breastfeeding is easy (I did it because it is soooo convenient; you never have to mix formula; it’s always the right temperature and amount) or it is hard (I never gave up even though my nipples were bleeding, my baby was screaming from hunger, I nursed every 2 hours and pumped every hour in between).
Lactivists have a similar problem with formula. It’s easy (don’t give women formula samples or they’ll use them because it’s easier!) or hard (all those bottles to wash! it’s so expensive!).
So which is it? Is breastfeeding easy or is it hard?
My theory is that the real dichotomy for natural childbirth advocates isn’t easy/hard, but right/wrong. Vaginal birth is “right” and C-sections are “wrong” and they will say whatever it takes to shame women into doing things the “right” way. So choosing a C-section is sometimes easy, sometimes hard, but always wrong. Similarly choosing to formula feed is sometimes easy, sometimes hard, but always wrong.
In both cases, advocates will say whatever it takes to sway the listener since advocates couldn’t care less whether a C-section or formula is easy or hard for a particular mother. They don’t care about her and they don’t care about her baby. They care only about themselves and their desperate need to validate their own choices by having everyone else mirror them back.
The truth is that individual women have individual circumstances that make individual choices easy or hard for them. Natural childbirth and lactivism have no room for individuality; they are all about conformity. Hence the ultimate ideological inconsistency: childbirth is natural, but you must read books, websites, hire a childbirth educator to teach you and a cheerleader (doula) to encourage you, use a birth ball, live blog and live tweet the event, hire a photographer and post the video on YouTube … just like they did in nature.

According to Peggy O’Mara, Editor of Mothering.com:
One source that does not have a conflict of interest is the Cochrane Collaboration, internationally recognized as the highest standard in evidence-based healthcare reviews. When Cochrane compared the midwifery model of care to other models of maternity care, they concluded “that most women should be offered midwife-led continuity models of care…” Cochrane also says that there is no strong evidence to favor either planned homebirth or hospital birth.
O’Mara is wrong.
O’Mara is not alone in her reliance on Cochrane Reviews. Lay people love Cochrane pregnancy and childbirth reviews. They always include easy to understand plain language summaries and are generally written by volunteers, many with an natural childbirth ax to grind.
To understand why Cochrane Reviews, particularly childbirth reviews, are often a poor standard of evidence, it helps to understand what Cochrane Reviews are and what they are not. Cochrane Reviews are systematic analysis of randomized controlled trials on a particular topic. Randomized controlled trials (RCTs) are trials in which two treatment options assigned randomly to two groups and in ideal cases neither the patient nor the scientist knows what treatment the patient received (double blind). RCTs are considered the “gold standard” in scientific research.
But what happens when RCTS are either unfeasible or unethical or both? For example, it is unethical to ignore women’s preferences and randomize them to home or hospital birth. Does that mean that it is impossible to investigate the relative safety of home and hospital birth? No, it does not. While RCT’s are at the top of the hierarchy of research methods, there are many forms of research including cohort studies, case-control studies and case series, among others.
But Cochrane Reviews do not consider these other forms of evidence, not because they are unreliable, but because they are outside the scope of Cochrane Reviews. That’s fine, but then they go ahead and do something that is not fine at all. When there are limited RCT’s or poor quality RCT’s, they analyze them anyway as if such an analysis could provide accurate data. Since it is unethical to perform an RCT on homebirth, there should be NO Cochrane Review of homebirth. Instead there is a review that is nothing more than garbage.
Here’s what the Cochrane Review of homebirth showed:
Main results
Two trials met the inclusion criteria but only one trial involving 11 women provided some outcome data and was included. The evidence from this trial was of moderate quality and too small to allow conclusions to be drawn. (my emphasis)
Authors’ conclusions
There is no strong evidence from randomised trials to favour either planned hospital birth or planned home birth for low-risk pregnant women.
No, there is no evidence PERIOD. Therefore no conclusion can be drawn PERIOD.
The bottom line is obvious. When it is unethical to perform RCTs or the RCT’s that exist are small and underpowered, a systematic review of RCTs is worthless. Hence the Cochrane Review of homebirth is useless.
Let me amend that: by publishing a “systematic review” that includes only 11 women, the Cochrane Childbirth Group makes it clear that they are willing to publish garbage if that is the alternative to publishing nothing at all.

Slate has published a terrific piece about C-sections written by Dr. Chavi Eve Karkowsky entitled Sorry You Were Tricked Into A C-section; What disapproving friends don’t understand about cesarean births.
Dr. Karkowsky perfectly captures the disdain and pity faced by women who have undergone a C-section:
You’d think any woman who has recently had major abdominal surgery and has a newborn to care for would have enough to deal with, but too often there’s more… A woman who has had a cesarean birth gets comments from her friends—online friends, IRL friends—mostly congratulations, but also messages of regret…
…[H]er friends and relatives tell her, outright or through subtext, that she must have been snookered. She was fooled and then underwent some shady butchery…
Dr. Karkowsky goes on to explain why these well meaning friends and relatives are often wrong. C-sections save tens of thousands of live in this country alone, each and every year.
I enter an operating room to do an unscheduled cesarean birth with gratitude… How lucky are we—how lucky is this mother and this baby, but also, selfishly, me—that we have another way. How lucky that I walk into that operating room reasonably sure that all three of us will come out, breathing, at ease.
So where did these “well meaning” friends and relatives get the idea that C-section are unnecessary? If you want to know the answer, follow the money. The money will lead you to an entire industry devoted to demonizing C-sections for its own economic benefit: the natural childbirth industry.
“Big Birth” is a multi-billion dollar industry, comprised of midwives, doulas, childbirth educators, and lay people who offer dubious services like placenta encapsulation. They have industry foundations and groups, complete with lobbyists and public relations people, devoted to promoting the economic well being of their members. Recognizing that it is rather crass to straightforwardly promote your own employment prospects, “Big Birth,” like other industries, presents itself as piously concerned with what is best for its customers. Big Oil just wants its customers to have access to the “best” method of heating their homes; Big Pharma just wants its customers to have access to the “best” medications; and Big Birth just wants its customers to have access to the “best” form of birth, vaginal birth.
There are plenty of goods and services that Big Birth can provide, but there are two that it cannot and both, therefore, threaten its economic bottom line. Those services are epidurals and C-sections and both are demonized with passion.
“Big Birth” demonizes epidurals despite the fact that there is no evidence – zip, zero, nada – that pain relief in labor is anything but beneficial for those who want it. But the effort to demonize pain relief in labor (“It’s good pain!” “Real women embrace the pain!” You won’t bond with your baby if you don’t feel the pain!”) pale in comparison to the frantic efforts to demonize C-sections.
C-sections dramatically cut into the profits of Big Birth so they must be caricatured as unsafe, unnecessary and positively harmful. When friends and relatives tell a C-section mother “outright or through subtext, that she must have been snookered. She was fooled and then underwent some shady butchery,” they are channeling the propaganda of Big Birth. Big Birth has been so successful in promoting their own economic self-interest, that their propaganda has become “conventional wisdom,” despite an almost complete dearth of scientific evidence to support their claims.
Birth Birth has been aided immeasurably by two factors. The first is the alliance with those who wish to save money by denying care, whether that care is necessary or not. Cesareans cost more than vaginal birth. Big Birth provides public relations cover for those who want to reduce the cost of obstetric care. Demonizing C-sections serves the economic bottom line of cost cutters and of Big Birth.
The second factor is that the late Marsden Wagner, MD, a diehard partisan of Big Birth, managed to gain a position of influence in the World Health Organization back in the 1980’s. Dr. Wagner almost single handedly engineered the now discredited WHO claim that the optimal C-section rate is between 5-15%. The claim was withdrawn in 2009 when the WHO acknowledged that there was no evidence and there HAD NEVER BEEN ANY EVIDENCE to support any optimal C-section rate, let alone the one decreed by Dr. Wagner. Indeed, international data shows that C-section rates under 15% are accompanied by unacceptably high levels of maternal and perinatal mortality.
Apparently the WHO was embarrassed by the way that it had been snookered and therefore buried its retraction in the middle of a large document leaving most people unaware of the retraction. Hence the claim continues to be repeated despite the fact that it was never true and has since been disavowed.
Are there too many C-sections? Possibly, and we should always be researching ways to lower C-section rates as far as we can without compromising safety. But the fact is that the countries with the best maternal and perinatal mortality rates have an average C-section rate of 22%, and very high C-section rates (up to 42% or more in the case of Italy) are completely compatible with excellent maternal and perinatal outcomes.
Some people have been snookered, but it isn’t the mothers who give birth by C-section. It is those who promote the idea that most C-sections are unnecessary, done for doctor convenience and harm mothers and babies, who have been fooled.
Follow the money. Those whose bottom line is threatened are the most vocal in demonizing C-sections. Big Birth is a huge industry, and like any industry, we should take their claims with not simply a grain of salt, but an entire shaker.