Call me old fashioned, but when I think of a successful birth, I think of a healthy mother and a healthy baby.
Apparently that’s not the case for the folks at the International Cesarean Awareness Network (ICAN), an organization that appears to think that the only successful birth is one that involved transit through the vagina … whether the baby was dead or alive.
Consider their post New Survey Shows High Success Rate for VBAC’s at Home. They are talking about the results of the statistics paper from the Midwives Alliance of North America:
Within this cohort were 1054 women with a history of cesarean section who were planning a vaginal birth after cesarean – VBAC – at home. (This is also referred to within the birth community as “HBAC” – home birth after cesarean). Within this subgroup, 87% had successful vaginal births, with 94% of those births occurring at home and the remaining 6% occurring after a transfer to a local hospital. This success rate is substantially higher than the 60-80% success rate reported across other large hospital-based cohorts (2) and likely reflects the high level of commitment to and support of natural birth, both from the mothers and their care providers.
If you are old fashioned like me, you might think that meant that there was a high rate of healthy babies who arrived by VBAC (vaginal birth after cesarean).
You would be wrong.
For those at ICAN, who are more concerned to boast about the use of their vagina than whether their baby survives, a dead baby is a “success” so long as a C-section wasn’t involved. It’s not that ICAN is unaware of the dead babies:
In the cohort reported by MANA, the intrapartum fetal death rate was significantly higher for women with prior cesarean compared to those without a history of cesarean (2.85/1000 versus 0.66/1000). For comparison, neonatal death rates for repeat cesarean and hospital VBAC were 1.03/1000 and 0.84/1000 …
Notice that nifty sleight of hand here (committed by MANA and repeated by ICAN), comparing FETAL death rate of the MANA cohort with NEONATAL death rate of the hospital group. The overall death rate in the MANA VBAC group was 5/1000. That’s a death rate 5X higher than comparable risk women giving birth in the hospital.
We at the International Cesarean Awareness Network (ICAN) find these statistics encouraging and applaud the Midwives Alliance of North America for collecting and presenting this data.
Encouraging??!! Anyone who is considering VBAC should take note:
When ICAN tells you that you have a high chance of a successful VBAC, they do not mean that your baby will survive. If you care about whether your baby lives or dies, you should be getting your VBAC information elsewhere.
The folks at ICAN and have nothing on the geniuses at the Midwives Alliance of North America, though. ICAN merely misrepresents the data and includes dead babies among “successful” VBACs. The fools at MANA don’t even understand their own data.
Consider this bit of appalling stupidity, direct from the MANA Facebook page (deleted the following day), in response to the observation that a VBAC death rate of 1/200 is hideous:
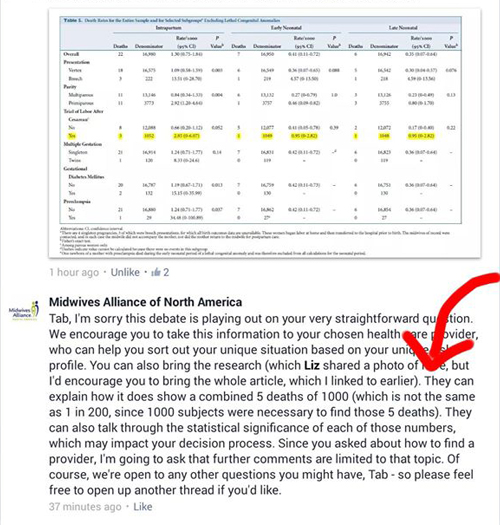
Here’s the money quote:
…[I]t does show a combined 5 deaths of 1000 (which is not the same as 1 in 200, since 1000 subjects were necessary to find those 5 deaths).
5/1000 is not the same as 1/200??!! 5/1000 is better than 1/200 “since 1000 subjects were necessary to find those 5 deaths”??!!
Those who rely on MANA for their information on the safety of homebirth take note:
If the people at MANA cannot do basic division, you cannot trust them to analyze their own data properly, let alone report it honestly.
It’s pretty clear that you cannot trust either ICAN or MANA to care about the safety of your baby.
Of course if you care about the safety of your baby, you wouldn’t be contemplating a VBAC at home in the first place, would you?