I’ve explained many times how I obtained the CDC mortality statistics for homebirth and hospital birth. People still have questions, so I made a video to demonstrate how to use the database.
Category Archives: Uncategorized
New Cornell study shows homebirth has 4X higher death rate than comparable risk hospital birth
The hits (to the safety of homebirth) just keep on coming.
The latest study, to be presented this Friday in New Orleans at the annual meeting of the Society for Maternal-Fetal Medicine, is titled Term neonatal deaths resulting from home births: an increasing trend.
The study was performed by analyzing CDC data, in exactly the same way that I have been analyzing it for the past 5 years. In this case, the authors chose to remove congenital anomalies as well.
There were a total of 10,453,778 term deliveries between 2007 and 2009 which met study criteria: 9,526,450 (91.13%) were by hospital physicians, 826,543 (7.91%) by hospital midwives, 30,415 (0.29%) by midwives in freestanding birthing centers, 48,202 (0.46%) by midwives at home, and 22,168 (0.21%) by others at home. NNM for those delivered at home by others and by midwives, and those delivered in a freestanding birthing center was significantly higher than those delivered by midwives in the hospital: hospital midwives: 3.1/10,000 (RR:1); home others: 18.2/10,000 (RR: 5.87; 95%CI: 4.21-8.19), home midwives: 13.2/10,000; (RR: 4.32 95%CI: 3.29-5.68), freestanding birthing center: 6.3/10,000;(RR: 2.03; 95%CI: 1.28-3.24)…

Amos Grunebaum, the lead author, was interviewed by Live Science:
For first time mothers, midwife-attended home births had even worse outcomes: 21.9 babies died for every 10,000 births. Risks also increased for older women, and women who were at 41 weeks of pregnancy, meaning they were more than a week past their due-date, Grunebaum said…
Unlike in the Netherlands, where all home birth attendants are professionally trained, home birth attendants in the United States may be inadequately trained, Grunebaum said.
In addition, home birth attendants in the United States don’t have firm criteria limiting which patients they should see, and so they may attend deliveries for high-risk pregnancies.
“They take twins, they take women who have prior C-sections, they do home deliveries in breech babies,” Grunebaum told LiveScience.
But even when looking at low-risk patients, home births are riskier, Grunebaum said. That’s because even a simple, uncomplicated birth can turn into an emergency very quickly.
“When the baby is in trouble, you have literally minutes to deliver this baby,” Grunebuam said. “There’s no time to transfer the patient from the home to the hospital in sufficient time.”
Women who want fewer medical interventions during labor or delivery, but still lower the risks for their babies should consider having trained midwives attend their births in a hospital, Grunebaum said.
It is important to understand that this study includes only PLANNED homebirths, and UNDERCOUNTS the actual risk of death at homebirth in 3 separate ways:
- Transfers to the hospital during attempted homebirth ended up in the hospital group and were not counted in the homebirth death rate.
- Intrapartum stillbirths are not included in this data, so homebirth deaths are undercounted even further.
- The authors of this study looked at all races, but white women account for more than 90% of women choosing homebirth, and the neonatal death rate for white women is much lower than that for all races.
Once again, we find that the dramatic increased risk of death at US homebirth is a remarkably robust finding. No matter where you look, whether it’s at state data like that of Oregon (9X higher), CDC data or even MANA’s own database (5.5X higher), midwife attended homebirth has a risk of neonatal or perinatal death anywhere from 3-9X higher than hospital birth.
What MANA found; what MANA did.
The following is from a comment taking issue with Judith Lothian’s post on the Lamaze blog Science and Sensibility praising the MANA study Outcomes of Care for 16,924 Planned Home Births in the United States: The Midwives Alliance of North America Statistics Project, 2004 to 2009. The authors claimed that the study shows homebirth is safe, but it actually shows that homebirth has a death rate 450% higher than comparable risk hospital birth.
This “study” brings up more questions than answers. And I hope MANA seeks to find answers – true answers, and not unfounded self-promoting headline – regarding the safety and risks of OOH birth…
Does MANA reviews these findings, identify clear risk factors that increase risk of death, and set professional standards for safe practice – based on their own research? Why or why not?
… The authors allude to insufficient collaboration between midwives and medical providers – is there any evidence in this sample to support this assertion? Case reviews of each incidence of perinatal death may illuminate this subject.
In this sample, was there any difference in outcomes between midwives practicing in states where CPMs are licensed and in states where they are not?
In this sample, were there individual midwives who had significantly higher perinatal mortality rates in their own practices? If so, what was there any common denominator among these types of midwives?
Let’s start asking the hard questions. Let’s start coming to conclusions about what makes midwifery and OOH birth safest and stop this nonsense of blind self-promotion. A group of health care professionals should adhere to ethical standards – first and foremost – to do no harm.
A question for homebirth advocates

Why would Melissa Cheyney, Wendy Gordon and other MANA executives spend 5 years hiding their own death rates if those rates showed homebirth was safe?
Can homebirth advocates offer any plausible reasons?
The many deceptions, large and small, in the new MANA statistics paper

Yesterday I gave a brief overview of the new MANA statistics paper (Homebirth midwives reveal death rate 450% higher than hospital birth, announce that it shows homebirth is safe) and pointed out that the fact that MANA waited 5 years to release the results demonstrates that Cheyney at el. have known for years that their death rates are hideous. It took them that long to figure out how to spin a death rate more than 5.5 X higher than comparable risk hospital birth as “safe.”
Today I’d like to take a closer look at the many deceptions, large and small, that Cheyney and colleagues have employed in writing a paper that has a conclusion directly opposed to the actual evidence.
But before we look at what Cheyney et al. wrote, it is helpful to consider what we need to know to make a determination of safety.
1. We need to know how many babies of the nearly 17,000 intended to be born at home actually died.
2. We need a comparison group. In this case, because we are looking at presumably low risk white women, ages 20-44, at term, with babies that are not growth restricted, the appropriate comparison comes from the Linked Birth Infant Death Files collected by the CDC. The database is publicly available on the CDC Wonder website. The death rate for the years 2004-2009 is 0.38/1000.
3. We CANNOT compare homebirth to out of date studies.
4. We CANNOT compare homebirth to other countries since the populations are quite different.
5. We CANNOT remove congenital anomalies from the homebirth group unless we also remove them from the hospital group.
6. We CANNOT assume that the fact that a baby died of a congenital anomaly at home means that it is a “lethal” anomaly. Many anomalies that inevitably result in death at home are highly treatable in the hospital.
7. We cannot remove breech, twins, VBAC, and other high risk conditions from the homebirth group because homebirth midwives are publicly on record claiming that these conditions are “variations of normal” and have lobbied across the country to have them included in homebirth midwives scope of practice.
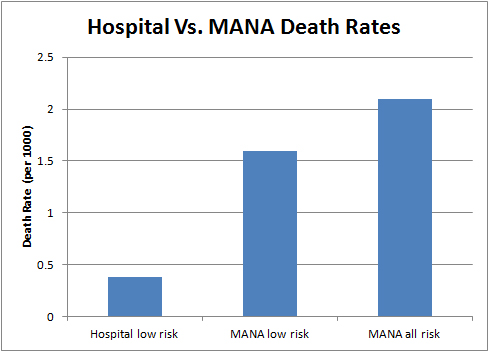
When we compare the death rate at homebirth of 2.06/1000 with the CDC death rate for low risk white women, ages 20-44, at term, with babies that are not growth restricted of 0.38, we find that homebirth has a death rate 5.5X higher than hospital birth. In other words, the death rate at homebirth is 450% higher than comparable risk hospital birth. A third way of expressing this finding is as follows:
4 out of 5 babies who died at home could have been saved in the hospital.
In simple terms, the bulk of the MANA stats paper is a bald faced attempt to bury these results by inappropriately removing groups that should be included and then inappropriately comparing the results to papers from other countries.
At various points in the paper, Cheyney et al. remove congenital anomalies, remove breech, twins and VBAC. They proceed to compare the result to homebirth papers from the Netherlands and Canada. They ignore the CDC death rates for comparable risk white women during the same years; indeed, to read the paper, you wouldn’t know that the CDC death rates exist.
Their conclusion:
If you inappropriately remove anomalies, breech, twins and VBAC and compare the results to homebirth studies from other countries, our results aren’t that much worse; ergo homebirth is “safe.”
Cheyney at al. do provide data that should give everyone pause:
Of the 22 fetuses who died after the onset of labor but prior to birth, 2 were attributed to intrauterine infections, 2 were attributed to placental abruption, 3 were attributed to cord accidents, 2 were attributed to complications from maternal GDM, one was attributed to meconium aspiration, one was attributed secondary to shoulder dystocia, one was attributed to preeclampsia-related complications, and one was attributed to autopsy-confirmed liver rupture and hypoxia. The causes of the remaining 9 intrapartum deaths were unknown.
So out of 22 babies who died during labor (compared to a predicted rate of zero deaths in the hospital), 13 died of preventable causes. They died because they were too far from the personnel and equipment who would have saved them.
For the 7 newborns who died during the early neonatal period, 2 were secondary to cord accidents during birth (one with shoulder dystocia), and the remaining 5 were attributed to hypoxia or ischemia of unknown origin. Of the 6 newborns that died in the late neonatal period, 2 were secondary to cord accidents during birth, and the causes of the remaining 4 deaths were
unknown.
So out of 13 babies who died in the neonatal period, at least 9 died of preventable causes. They died because they were too far from the personnel and equipment who would have saved them.
In other words, out of the 35 homebirth babies who died, at least 22 died of obviously preventable causes.
The death rates in certain subgroups were astronomical.
(5 fetal/neonatal deaths in 222 breech presentations), TOLAC (5 out of 1052), multiple gestation (one out of 120), and maternal pregnancy-induced comorbidities (GDM: 2 out of 131;
preeclampsia: one out of 28
The authors are honest about the primary methodological limitation of the study. Data collection was voluntary and only 20-30% of CPMs contributed:
The main limitation of this study is that the sample is not population-based. There is currently no mandatory, reliable data collection system designed to capture and describe outcomes for all planned home births in the United States.We are also unable, for a number of reasons detailed elsewhere, to quantify precisely what proportion of practicing midwives of various credentials contributed data to MANA Stats between 2004 and 2009…
It is highly likely, therefore, that the 450% elevated death rate dramatically UNDERCOUNTS the real risk of homebirth.
Nonetheless, we can reach important conclusions. Despite the fact that the authors surveyed only a small proportion of practicing midwives, who submitted data that was not validated, and despite the fact that they authors performed a variety of maneuvers that violated basic standards of statistical analysis, and despite the fact that they were intent on concluding that homebirth is “safe” regardless of what the data showed, they actually showed that homebirth has a minimum rate of death 5.5X higher than comparable risk hospital birth.
We can also be sure that the authors understood that their data showed that homebirth has a horrifically high death rate, because they try to hide the number of deaths for the past 5 years, released the data only under pressure, and then proceeded to draw a conclusion entirely at odds with what their own data showed.
In addition, we can also conclude that homebirth is NEVER appropriate for breech, twins or VBAC.
Finally, we can come away from the paper with the horrifying realization that MANA has absolutely no idea what its own members are doing. There is no systematic attempt to determine if they are safe practitioners. To hear the authors tell it, they can’t even figure out how many practicing CPMs are actually submitting statistics, let alone whether those statistics are accurate.
When it comes to the safety of homebirth, the only question remaining is:
Who are you going to believe, MANA or your own eyes?
Homebirth midwives reveal death rate 450% higher than hospital birth, announce that it shows homebirth is safe.
Why did the Midwives Alliance of North America wait 5 years to publish its statistics?
Why did the Midwives Alliance of North America wait 5 years to publish its statistics?

There’s so much to say about the new MANA study by Cheyney et al. that I’ll be covering it in several posts.
Earlier today I gave a brief overview of the results (Homebirth midwives reveal death rate 450% higher than hospital birth, announce that it shows homebirth is safe). In this post, I’d like to address the timing of publication of this study.
Specifically, if the results of the study really show that homebirth is safe, why did MANA wait 5 years to publish them?
The answer is that the study doesn’t show that homebirth is safe and Cheyney et al. are fully aware of that fact. They didn’t want to publish the results, but they were pressured into it, and are now trying to convince people that a death rate more than 5.5 X higher than comparable risk hospital birth is “safe.”
Their reluctance to publish damaging data is known in technical terms as publication bias.
MANA did not pioneer this type of publication bias. That was done by the drug companies. They have a vested interest in publishing studies that promote the use of their medications and failing to publish study results that call the efficacy or safety of their drugs into question. The classic case of this type of publication bias is Vioxx. Merck had commissioned and paid for a study that showed Vioxx had dangerous side effects. Merck did not publish these results and did not share them with physicians.
How do we know that the failure to publish the MANA statistics for the past 5 years was publication bias? Since we are not privy to the thought processes of the investigators, we can only tell by process of elimination.
The failure to publish was not due to the lack of availability of the statistics: As early as the summer of 2006, MANA was offering the statistics up through the previous year … but only to people vetted by MANA who were willing to sign a non-disclosure agreement promising not to let anyone else see the results.
The failure to publish the results was not due to a need to withhold the data pending journal publication: As far back as April 2011, MANA was publicly boasting about the 5% C-section rate in this cohort. But they wouldn’t tell anyone how many babies died to achieve that C-section rate.
The failure to publish was not due to any need to publish them in the context of research: I had been pounding MANA on my blog about the failure to release their death rate since 2006, but it wasn’t until November 2011 that I gained a large national readership with my piece in Time.com. The executives at MANA were so alarmed that they felt the need to respond publicly.MANA executives implied that statistics could only be released in the context of research. That is completely untrue. Every state and the US government releases annual statistics on the number of births and the number of neonatal deaths (not to mention a myriad of other health issues). This information is publicly available to anyone for free through the CDC. MANA could have released its data to the public for free in the same form as the CDC data. There was nothing preventing them from doing this beside their unwillingness to reveal the numbers.
MANA has been quite creative in fabricating new excuses: In October 2013, Melissa Cheyney claimed that MANA could not release its statistics without IRB approval. That’s not true. First, MANA itself has published almost all the data from the database EXCEPT the death rates. Second, while IRB approval could be required for publications based on the data, IRB approval is not required to read and review the data.
It’s difficult to conclude that MANA had any other reason for holding back the statistics besides the fact that they KNOW this data shows that homebirth has a dramatically increased risk of death.
Why did they suddenly relent and publish the data?
I suspect that there were two reasons.
First, increased public pressure such as the Change.org petition demanding the release of the data.
Second, their failure to publish the death rates had led everyone to the obvious conclusion that the death rates were hideous. Therefore, I suspect that they gambled that they had nothing to lose by publishing the data and then pretending it shows something different than what it actually shows. Everyone already knew that the death rates were horrible so the only way to combat that impression was to publish them and slice and dice the data in a million ways to confuse readers, while simultaneously misrepresenting what the death rates mean.
Simply put, MANA refused to release the death rates until now, because they know and have always known that these death rates are horrific. If the death rates were even close to demonstrating safety, MANA would have been shouting them from the roof tops since 2006, when the first analysis was complete. Instead they waited until they were pressure to release the data and are now hoping to hoodwink their followers by declaring that a 450% increased risk of death at homebirth is an indication of safety.
The only thing that remains to be seen is whether their followers are gullible enough to ignore the evidence of their own eyes in favor of the deliberately misleading spin put forth by MANA.
If any homebirth advocates have another remotely plausible reason why MANA withheld data of “safety” for the past 5 years, while publicly releasing every the C-section rate, the intervention rate, the transfer rate, etc. etc. etc., I’d love to hear it … but I’m not holding my breath because I could turn mighty blue.
Homebirth midwives reveal death rate 450% higher than hospital birth, announce that it shows homebirth is safe.
The many deceptions, large and small, in the new MANA statistics paper.
Homebirth midwives reveal death rate 450% higher than hospital birth, announce that it shows homebirth is safe
True to form, the Midwives Alliance of North America continues its deceptions about the risk of death at homebirth.
For the past 5 years, I have been relentlessly publicizing the fact that the Midwives Alliance of North America (MANA) has refused to release their own death rates. It doesn’t take a rocket scientist to realize that the death rates must be hideous, AND recognized as hideous by MANA executives.
After 5 years, and mounting pressure, MANA finally decided how to spin their hideous death rate: pretend that the hideous death rates aren’t hideous!
Isn’t that clever?
They are hoping that journalists will print their bogus conclusion, instead of the actual numbers.
The papers themselves are due to be released later today (at which point I will analyze them in depth), but the press releases include some of the numbers so we can take a look at them now.
According to Citizens for Midwifery:
The overall death rate from labor through six weeks was 2.06 per 1000 when higher risk women (i.e., those with breech babies or twins, those attempting VBAC, or those with preeclampsia or gestational diabetes) are included in the sample, and 1.61 per 1000 when only low risk women are included. This rate is consistent with some published reports of both hospital and home birth outcomes, but is slightly higher than others.
No, it isn’t “slightly” higher. It is MASSIVELY higher.
According to the CDC Wonder database, the neonatal death rate for low risk white women at term from the years 2004-2009 is 0.38/1000. As Judith Rooks, CNM MPH noted in her review of Oregon homebirths, intrapartum death among low risk babies is essentially non-existent in the hospital, so the neonatal + intrapartum death rate for the hospital is still 0.38
As the chart above demonstrates, the MANA death rate for the same years was 5.5X HIGHER. In other words, the MANA death rate was 450% higher than the hospital death rate.
On what planet is a death rate 450% higher than expected a safe outcome? Not on this planet.
MANA and homebirth midwives have been lobbying extensively for a scope of practice that includes breech, twins, VBAC, etc. Now they want to exclude those same births from their statistics. Even then, the MANA death rate is 4.2X higher than hospital birth. So even when homebirth midwives stick to low risk patients, homebirth has a death rate 320% higher than comparable risk hospital birth.
That’s hardly a safe outcome, either.
The results for various risk factors are even more appalling.
Of 222 babies presenting in breech position, 5 died either during labor or the neonatal period.
So the homebirth death rate for breech was 20/1000 compared to approximately 0.8/1000 in the hospital. That’s a breech death rate 25X higher (2400%) than the hospital.
To summarize, the MANA statistics show that homebirth as practiced in the US has a death rate 450% higher than hospital birth.
No wonder MANA has been hiding these numbers for years.
Why did MANA wait 5 years to publish its statistics?
The many deceptions, large and small, in the new MANA statistics paper.
MicroBirth?

Homebirth and natural childbirth advocates keep throwing memes against the wall, hoping one will stick.
Obstetricians don’t follow scientific evidence! Except that they do.
The media is to blame for the pain of childbirth! Except that it isn’t.
Homebirth is a human right! Except that it’s not.
A healthy baby isn’t enough! Except that for most women, it is.
My personal favorites, though, are the pitiful attempts by homebirth and natural childbirth advocates to harness to their cause scientific disciplines about which they clearly are ignorant. Their invocation of quantum mechanics and chaos theory aren’t merely pitiful, they are hilarious.
Now they’re about to throw a new meme against the wall: MicroBirth.
That’s the breathless announcement from One World Birth, the same clowns who nominated Lisa Barrett, a one woman birth-crime wave, as a “National Birth Hero.”
What is MicroBirth?
Over the past three years we have been on a journey, trying to connect the pieces of the jigsaw puzzle that is birth…
The more we discovered, the more convinced we were that there was a vital piece missing from the picture.
A piece that connected everything…
The reason it has proved to be so elusive for so long is because it is not visible to the naked eye.
It is microscopic.
What does that mean?
It is supposedly:
… brand new science investigating crucial microscopic events that occur during and immediately after birth.
And, more importantly, what happens when the natural processes of childbirth are interfered with or bypassed completely…
[I]ncreased medicalization of childbirth may be having severe consequences on the life-long health of our children.
What’s more, it could be having a devastating effect on the future of our entire species.
Holy hyperbole, Batman! What could it be?
They don’t say, but I have a guess. I’m going to guess that it’s another pitiful attempt to harness cutting edge scientific disciplines about which they are painfully ignorant, in this case epigenetics and the microbiome.
For those who have no idea about the science of the microbiome and the science of epigenetics, such an effort makes perfect sense:
Natural childbirth and homebirth advocates have a massive problem. The scientific evidence does not support their claims. Natural childbirth isn’t safer and hombirth isn’t safe at all. You might think that would cause them to re-evaluate their core beliefs, but you’d be wrong. Natural childbirth and homebirth are cults, and their core beliefs are non-falsifiable. Therefore, they must abandon their original claims that natural childbirth and homebirth are visibly safer. No problem! Natural childbirth and homebirth are safer on the microscopic scale!
We’ve already seen a preview of this approach. In January 2012, a group of midwives convened a panel on Epigenetic Influence and Impact on Childbirth.
Hannah Dahlen, an Australian midwife, says it could increase respect and demand for vaginal birth. “We’re at the beginning of a very exciting time,” Dahlen says. “I think in 10 years we will potentially look back at what we are doing now and think, ‘What on earth did we do?’” …
They were all frustrated “that despite the research, political activism and efforts they and many others were putting in to increase the rate of normal birth, intervention during childbirth kept rising and arguments about safety and outcomes all had a short term focus,” she wrote in an email.
How frustrating that obstetricians and mothers are focusing on the such short term outcomes as whether the baby lives or dies, is born intact or has suffered a brain injury. Sure, childbirth interventions like C-section make childbirth safer on the macro level (duh!), but at the level of DNA, interventions cause severe consequences on the life-long health of our children (only the ones who survive childbirth, of course) and OUR ENTIRE SPECIES!!!
And not only that, but childbirth interventions might change to microbiome of the gut cause severe consequences on the life-long health of our children (only the ones who survive childbirth, of course) and OUR ENTIRE SPECIES!!!
There’s just one teensy, weensy problem. THERE IS NO EVIDENCE TO SUPPORT THOSE CLAIMS.
Epigenetic changes, the chemical modifications of DNA that are the result of environmental influences, are the results of long term events lasting months or years, like famines. There’s not a shred of evidence that ultrashort term events like childbirth cause ANY changes to DNA, let alone deleterious changes.
Similarly, there is not a shred of evidence that altering the microbiome of the gut of the newborn (if indeed such alterations occur) has any long term impact on health.
But wait! Childbirth interventions and C-section rates have been rising steadily and look at the long term impact on health! Since the advent of modern obstetric interventions …. we live longer and healthier lives than ever. Oops!
I predict that this meme isn’t going to stick, either. First of all, “More babies die at homebirth, but the ones who live have better genes!” and “More babies die at homebirth, but the ones who live have better gut bacteria!” are not like to be an effective rallying cries. Second, the central premise, that obstetric interventions are safer on the macro level but cause long term microscopic health problems is obviously nothing more than nonsense.
Natural childbirth and homebirth advocates are (once again) making themselves look like fools, while failing to advance their cause in any meaningful way. They are simply flailing around trying desperately to justify a failed philosophy that has put, and continues to put, the lives of babies at risk.
Because, really, who wouldn’t want to have sex right after giving birth?

It is almost impossible to parody homebirth advocates because they are so busy parodying themselves.
Case in point, the latest masterpiece from Serge Bielanko, 5 Reasons I’m Excited About Our Home Birth.
You may remember Serge. He’s the guy who apparently thinks it’s simply hilarious that people are warning him about the increased rate of death and brain injury at homebirth.
What words of wisdom does Serge have for us this time? He shares his top 5 reasons for looking forward to his wife’s upcoming homebirth. Amazingly, meeting the baby isn’t on his list.
That’s not really surprising when you consider that homebirth isn’t about the baby and it isn’t even about birth. It’s about parents and their self-image. The baby might live, the baby might die, but that’s not what’s important. Serge and his wife want you to know that they are crunchy hipsters, daringly transgressive and oh, so, sexy.
The piece is howlingly funny, albeit unintentionally. What are the 5 things that Serge is looking forward to that give meaning to risking his baby’s life for nothing more important than bragging rights.
1. Anyway She Wants It: I love the fact that, after a long and arduous pregnancy, my wife, Monica, will be able to not only experience a natural labor unlike she experienced with the medically-induced births of our other two kids, but she’ll also be able to direct the show, so to speak.
Because, as we know, homebirth is a piece of performance art with the mother as the star and the baby as a prop.
2. The Vibe: Obviously, most hospitals will allow you to keep the blinds shut in the room when you’re in there to have a baby. And if you want them raised wide open, well, they’re typically OK with that, too. But beyond those kinds of things, you don’t always have the liberty to control the vibe in a hospital delivery room.
Is this fool for real? The vibe?
Candles, music, dark intimate rooms … man, the way we are looking at our home birth is such a turn-on that we could very possibly end up having another baby precisely nine months to the day after this one arrives, if you know what I’m saying.
Because, really, what woman wouldn’t want to have sex right after giving birth?
3. Less is More: … But, after two birth experiences in hospitals, I believe I can honestly say that the circus-like atmosphere that occurs in a lot delivery rooms can be a real turn-off, and maybe even an impediment, for a woman in labor. There is nothing peaceful or tranquil about it, really. There are people coming in and out all of the time, and the notion of being alone with your thoughts and your energy and the one or two people you love and trust and want to share the birth with, all of that is blown to bits by the constant barrage of monitoring nurses and physicians and other assorted absolute strangers.
Serge, let me tell you a secret. When your baby’s life is at risk, and it’s at risk in any birth, less may be NOT ENOUGH!
And you know what could really blow your thoughts and your energy to bits? Raising a brain injured child who can’t walk, talk and play like the other kids because you and your wife were more interested in your “thoughts and energy” than whether the baby’s brain got enough oxygen.
4. Connection: I’m sure it isn’t the first thing on anyone’s mind when they think about having a baby and all, but truth be told, the actual labor and arrival of a child into this world is a magnificent opportunity for the two people who created him or her to cash in on the kind of bonding that happens across the course of that special day, maybe even across just a few hours, but that perseveres and lasts for the rest of a lifetime.
Serge, this is obviously going to come as a major shock to you, but strong emotional bonds don’t require privacy. When my husband kissed me under the marriage canopy more than 30 years ago, our bond was immeasurably strengthened, not despite the presence of more than a hundred guests, but because we were celebrating our emotional bond in front of the world.
I’m must admit I am really beginning to feel sorry for homebirth advocates. They are so limited in their ability to bond with their own babies that something as trivial as having an epidural impacts their bonding. In contrast, I and most of the other parents I know have a bond of love with their children that is so strong that even our own deaths won’t break it.
5. Wine: Before you hasten to judge me on this one, let me just say two things.
First off, the wine is for me, the dad, a guy who seriously loves his kids and his wife and is ultra-excited to welcome a baby into this world in the same old and ancient way that he likes to welcome all sorts of good things into his life: with a glass or two of Rioja or Cabernet Sauvignon.
Secondly, if, by chance,you are the type of person who kind of steps back in horror at the mere mention or idea of someone sipping an adult beverage while a baby is being born, let me just say this much.
Go to the hospital.
That’s the way they do things over there; no mood lighting, no serenity, no intimacy, and no wine.
Oh, the horror!!
Serge, here’s a little unsolicited advice: GROW UP!
Giving birth is not about you, it’s about the baby.
Being the parent means putting the life (and brain function) of your child AHEAD of your immature fantasies of creating the perfect performance (and, apparently, having sex immediately thereafter). Get a grip! You’re not transgressive; you’re not hip; you’re not educated. You’re selfish and self-absorbed, boasting about acting like a fool.
And that’s a shame. You are about to participate in a wondrous event and the sad thing is that you are so busy worry about yourself, how you look, how you feel, whether or not everything is exactly to your liking that you can’t appreciated the miracle that is the BABY!
You remember the baby, right?
Or maybe you don’t.
Instead of Birth Without Fear, how about Birth Without Death?

I wonder how many women have been supported and encouraged by homebirth websites to risk their babies’ lives at homebirth and then have those babies die.
Here’s one mother:
I love my intuition to find a midwife and I love the fact I have the strength to attempt a home vba2c …
I’m having a vba2c in nov with a homebirth midwife, I must say I trust my midwife with my entire soul, the amount of knowledge and experience a good midwife has is far far far more superior to an obgyn , since the obgyn is a sergeon [sic] they will of corse be more comfortable to reccomend such intervention. Your body can do it …
The picture of the dead baby on Stillbirthday:
My sweet son who left the body during labor , I miss him with my every breath …
The obituary.
The desperate attempt at rationalization:
I would like to heal from (emotionally/physically) _____________ (regarding pregnancy/birth/motherhood).
Losing my son (3rd child) at 43 weeks during labor , was attempting a home birth vba2c , his passing was NOT due to me attempting a vaginal birth or a home birth , in fact when we attempt to have our 4th child I will be going for a vba3c, I am so supported through this by the women in my local homebirth group , it has allowed me to see the sun in the storm, I have started a charity in my sons name to help women get a doula or midwife when they would not be able to afford their services other wise.
Instead of worrying about whether their babies are naturally born, or born without fear, homebirth advocates should concentrate on whether their babies are born alive. Then maybe they will be born alive.
Addendum: If that were not horrifying enough, the “healing” thread from Birth Without Fear contains yet another homebirth death that occurred only a few weeks before. His mother wrote:
I would like to heal from (emotionally/physically) _____________ (regarding pregnancy/birth/motherhood).
Emotionally from the death of my son at two days old (7 weeks ago). After a perfect pregnancy and labor, my son was born and didn’t breathe unexpectedly. He lived two days on life support, and then died in my arms when we let him go…
Apparently this was just another casualty of midwives’ efforts to bring third world causes of death to the first world. Just another homebirth baby who was “fine” right up until it dropped nearly dead into the hands of the clueless midwife … just like the other 18 homebirth babies I have written about in the past 3 years who died in the same way.
According to the midwife’s website:
Perfect pregnancy
Perfect parents
Perfectly loved
Perfectly wrong that you are gone so soon
And perfectly unnecessary. When will these women stop worrying about their “experience” and start worrying about whether their babies will live or die?