
Dr. Neel Shah owes a lot of women an apology.
I wrote yesterday about Dr. Shah’s endorsement of homebirth, both for Time.com and in this post.
My rebuttal of Dr. Shah’s claims was simple; he appeared to be entirely unaware of the published literature on the dramatically increased death rate at American homebirth, and equally unaware that homebirth in the US is typically attended by a second, inferior class of midwife, one who does not meet the basic education and training standards in any other industrialized country. Inexplicably, he was endorsing homebirth in the pages of the New England Journal of Medicine when he hadn’t read the basic literature.
Apparently stung, Dr. Shah sent me this unsolicited Tweet:
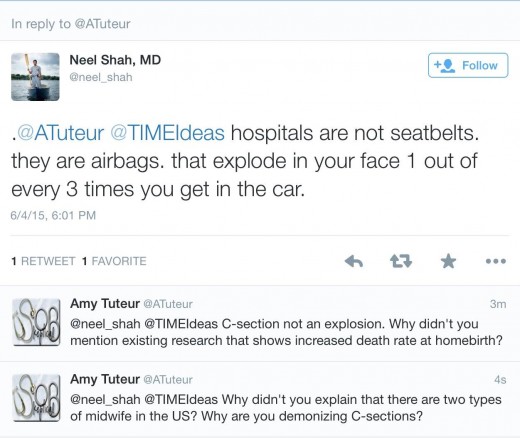
[H]ospitals are not seatbelts; they are airbags that explode in your face 1 out of every 3 times you get in the car.
I find that to be a ridiculous analogy, issued in an attempt to undermine the measured argument that I made.
I wrote:
Hospital births are like seatbelts. Most of the time you won’t be in a car accident so you don’t need them; but when you need them, they save lives. Just like failing to buckle your child in on a drive to the store in unlikely to result in that child’s death, homebirth is unlikely to result in the death of a child. But over large populations riding in cars repeatedly, routinely buckling seatbelts saves thousands of lives. When it comes to homebirth, each mother must decide whether she is willing to tolerate the risk to her baby of dying at homebirth, a risk that is higher than the risk of the same baby dying in a car accident.
Apparently Dr. Shah is referring to the American C-section rate of 32%. Talk about hyperbole! He implies that 100% of C-sections are unnecessary, and are performed merely because the system is malfunctioning spectacularly. At a MINIMUM, fully half of those C-sections he derides are medically necessary and a substantial proportion are literally life saving. Yet Dr. Shah implies that obstetricians are performing C-sections for reasons that aren’t merely illegitimate, but are a travesty exploding in the face of unsuspecting mothers. Dr. Shah owes American obstetricians an apology for that insinuation.
But I’d like to address a different issue:
What message are we sending to women when we deride their C-sections as airbags that “explode in your face”?
We are sending the message that women who undergo C-sections for whatever reason (Dr. Shah didn’t exclude medically necessary C-sections) are damaged, defective, and have been hoodwinked by evil obstetricians. In other words, we imply that women who have had C-sections ought to be ashamed of them and of themselves.
That’s an ugly, unjustified and unjustifiable message. This endless demonization of C-sections has got to stop. It is incontrovertible that C-sections have saved more lives than nearly an other procedure in modern medicine.
Is the C-section rate too high?
As someone who had a 16% C-section rate when I practiced, I believe that it is. Not because there is anything wrong with C-sections, not because C-sections cost “too much” and certainly not because vaginal birth is somehow better, since it isn’t it. I believe that we can safely lower the C-section rate somewhat by promulgating clearer, stricter indications.
Nonetheless, I have the deepest admiration and respect for women who undergo C-sections. Consider C-sections for fetal distress. In 2015, the diagnosis of fetal distress is imperfect at best:
…We know that almost all babies who experience lack of oxygen during labor will give evidence of that on electronic fetal monitoring. In contrast, many babies who appear to be in distress may actually be fine. When a woman consents to a C-section for fetal distress, she is saying in essence: I don’t know whether my baby is truly experiencing oxygen deprivation, but I don’t want to take any chances. Cut me and help the baby; if I’m wrong, it’s a price I’m willing to pay to be sure that my baby is okay.
In other words, its a sign of devotion, not a sign of failure. And it is NEVER a sign that they are damaged, defective or have been hoodwinked.
Dr. Shah owes C-section mothers an apology. In an effort to express his displeasure with me, he callously insulted them.
Not to mention his analogy is weak, incorrect and yet another example of the unreflective demonization of C-sections so beloved of those who can’t perform them and those who don’t want to pay for them.









{kind=link}