I guess this woman didn’t get the message that I have declared April to be Cesarean Appreciation Month.

This will ruffle feathers, it’s okay. I do not get celebrating c-sections. I’ve had two. They were awful. Neither of my children’s births were beautiful. They were horribly traumatic for them, and for me. I’m a full on attachment parenting, unschooling mom. You cannot be these things without celebrating your children everyday of their lives, and offering gratitude for them nearly every moment of everyday. Celebrating their assault while entering this world? Never.
Note: I am referring to the act of celebrating c-sections in general, not a particular one or ones.
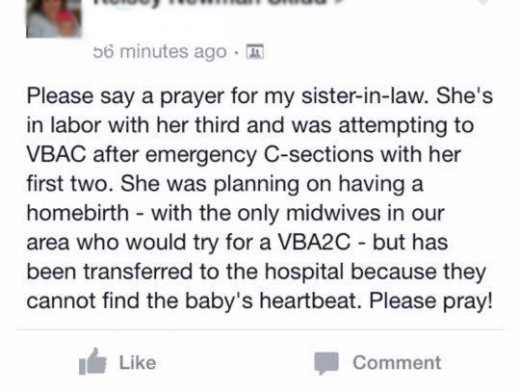
She doesn’t appreciate her C-sections, does she?
I left a comment:
“Disappointed in your C-sections? Blame the industry that set you up for disappointment, the natural childbirth industry. That’s the industry that encourage women to value process over outcome.
In the chapter The Dialectics of Disruption: Paradoxes of Nature and Professionalism in Contemporary American Childbearing, anthropologists Caroline Bledsoe and Rachel Scherrer examine why meaning-making is so important within the culture of natural childbirth advocacy.
Their description of the current situation:
‘… Birthing is depicted culturally as an individual achievement, one in which a woman should be in control of her actions. For this, women attempt to present themselves as professionals, medical as well as legal: as close as they can come to being equals with their medical peer doctors, informed and trained to evaluate their qualifications.’
Bledsoe and Scherrer recognize that meanings and meaning-making are luxuries of a society in which childbirth is so safe that women have forgotten that in reality it is inherently dangerous:
‘… As childbearing became safer and more benign visions of nature arose, undesired outcomes of birth for women came to consist of a bad experience and psychological damage from missed bonding opportunities. Today, with safety taken for granted, the new goal has become in some sense the process itself: the experience of childbirth…’
Their critical insight:
‘… But with *control* being such a crucial issue in cultural ideals of childbearing, the greater the expectations that a scripted birth plan creates, the greater the surety that the woman will fall short of her ideal. Some elements will go wrong, and with them the hope of remaining the equal of the professionals who deals with her birth. This relegates obstetricians, who have the power to disrupt a naturalism but also to save lives if something goes wrong, to being the inevitable targets of opposition.’
Specifically:
‘If nature is defined as whatever obstetricians do not do, then the degree to which a birth can be called natural is inversely proportional to the degree to which an obstetrician appears to play a role. The answer to why obstetricians are described with such antipathy thus lies not in the substance of what obstetricians do that is unnatural – whether the use of sharp incision. forceps, and medications that blunt sensation. or anything else- but in the fact that obstetricians represent a woman’s loss of control over the birth event. Obstetricians are thus perceived as the chief source of disruption in the birth event, backed by the licensing power of medicine and the law. And yet it is not what obstetricians do that women find problematic but the fact that they are the people who step in when the woman is seen to have failed.’
If the goal of childbirth is seen as a healthy baby, there’s no reason to be disappointed with a C-section. But if the goal is a carefully scripted, NCB approved birth “experience,” it’s no wonder that you are disappointed. The problem is that you blame the C-sections when you should be blaming the natural childbirth industry.”
She immediately deleted the comment. It was not offensive in the least, but I guess she couldn’t stand the cognitive dissonance of acknowledging that she had been set up for disappointment by the natural childbirth movement.
Or maybe she was just enjoying feeling sorry for herself and didn’t want anything to detract from her fine Cesarean whine.