When it comes to discrediting lactivism I get lots of help from an unlikely source, lactivists themselves.
For sheer viciousness, it’s hard to top Kathy Dettwyler, Associate Professor, Supplemental Faculty, Dept. of Anthropology, University of Delaware, Newark, who is known for her cultural work on extended breastfeeding and weaning. You may remember the nasty comment she left on a positive Amazon review of the book Lactivism:
[pullquote align=”right” cite=”” link=”” color=”” class=”” size=””]Lactivists can’t identify even a single term baby who suffered brain damage from properly prepared infant formula, yet they’re willing to risk brain damage from insufficient breastmilk.[/pullquote]
… Formula fed children definitely WILL BE INFERIOR to how those same individuals would have turned out if they had been breastfed.
Now she’s spewing drivel that is, if possible, even more offensive.
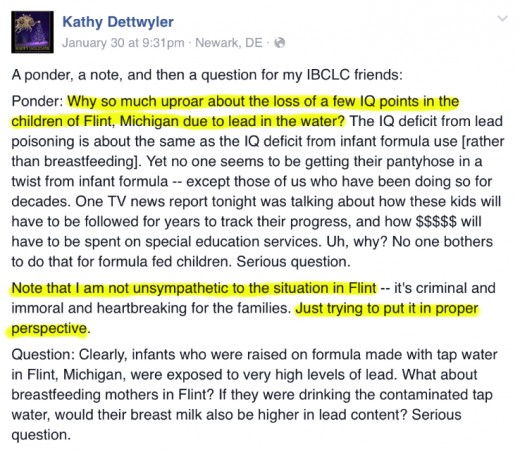
Ponder: Why so much uproar about the loss of a few IQ points in the children of Flint, Michigan due to lead in the water? The IQ deficit from lead poisoning is about the same as the IQ deficit from infant formula use [rather than breastfeeding]. Yet no one seems to be getting their pantyhose in a twist from infant formula — except those of us who have been doing so for decades. One TV news report tonight was talking about how these kids will have to be followed for years to track their progress, and how $$$$$ will have to be spent on special education services. Uh, why? No one bothers to do that for formula fed children. Serious question.
Note that I am not unsympathetic to the situation in Flint — it’s criminal and immoral and heartbreaking for the families. Just trying to put it in proper perspective…
It’s proper perspective? Yes, let’s put it is its proper perspective.
The effects of lead poisoning on the brain are manifold and include delayed or reversed development, permanent learning disabilities, seizures, coma, and even death.
See? Formula is exactly the same… Oops, guess not. But that doesn’t stop Dettwlyer from exploiting the tiny victims of lead poisoning to further her personal agenda.
Lest you think that the ugliness of lactivism is restricted to clowns like Kathy Dettwyler, consider the actions of Alison Stuebe, MD, a well known professional lactivist.
In a recent piece for the Academy of Breastfeeding Medicine blog, Of Goldilocks and neonatal hyponatremia, Dr. Stuebe felt compelled to address a petition that is circulating highlighting the dangers to babies of inadequate breastmilk.
A heart wrenching story has been circulating on social media about an exclusively breastfed baby who suffered brain damage after 4 days of ineffective feeding. The mother shares how she was reassured that all mothers can make milk, and did not realize until she engaged a lactation consultant at 96 hours postpartum that her child was profoundly dehydrated.
…That warning would directly challenge efforts across the US, and around the world, to emphasize the value of exclusive breastfeeding and the risks of unnecessary supplemental feeding.
Yes, just another random mother complaining about a random event…
Not exactly.
I commented on the post:
Dr. Steube, I notice that you display your own credentials prominently, but you disrespectfully ignored Dr. Christie del Castillo-Heygi’s credentials, referring to her as “the mother.” Dr. Castillo-Heygi is a practicing emergency room physician with degrees from Brown and UCSF medical school.
To her credit, after multiple complaints over 24 hours, including my suggestion to edit the piece, Dr. Stuebe did ultimately identify “the mother” and link to her story, but I wonder why Dr. Stuebe neglected to do so in the first place.
It’s not because Dr. Stuebe denies the deadly reality of neonatal hyponatremia; she doesn’t. It appears she didn’t want to give credence to Dr. del Castillo-Heygi’s experience and the lasting impact on her son.
Dr. Stuebe didn’t want to give attention to the risk of PERMANENT BRAIN DAMAGE and DEATH because she’s more concerned about the “risks” of unnecessary supplemental feeding. And what risks would those be? Not brain damage, not death, but the disruption of the breastfeeding relationship.
I suspect that Dr. Stuebe would be hard pressed to identify even a SINGLE term baby who suffered brain damage from properly prepared infant formula, yet she’s willing to risk brain damage from insufficient breastmilk. I suspect that Dr. Stuebe would be hard pressed to identify even a SINGLE term baby who died from properly prepared infant formula, yet she’s willing to risk infant deaths from insufficient breastmilk.
Dr. Stuebe offers a straw man fallacy to defend her point of view:
What, then, of the tragic stories of brain-damaged babies? Wouldn’t it be easier to supplement all babies, rather than redesign our systems of care to identify dyads at risk and ensure early follow-up for every baby?
No one, least of all Dr. del Castillo-Heygi, has ever suggested supplementing all babies.
Amidst the attempts at obfuscation, Dr. Stuebe admits:
We might start by acknowledging, once and for all, that not all mother-baby dyads are able to breastfeed exclusively. Reproductive physiology is not infallible. 10.9% of women have difficulty getting pregnant or carrying a baby to term. 15 to 20% of pregnancies end in miscarriage, 10% of infants are born preterm, and 1 in 100 infants are stillborn. Similarly, less than 100% of women can exclusively breastfeed.
Which, of course, has been Dr. del Castillo-Heygi’s point all along. Kudos to her for forcing the lactivist establishment to admit it.
Lactivists, both professionals and lay people, seem to have lost their minds over breastfeeding. The truth is that it’s just not that big of a deal. Breastfeeding has benefits, but in first world countries they are trivial, but the moralization of breastfeeding has paralleled the monetization of breastfeeding and an entire industry now believes that it depends on grossly exaggerating the benefits and misrepresenting the risks.
But it’s not all deadly seriousness. Here’s a tweet I received from a lactivist offended that I criticized the recent Lancet breastfeeding studies:

Hard to beat that for eloquence!