Both purveyors and consumers of alternative health believe in a lot of wacky things.
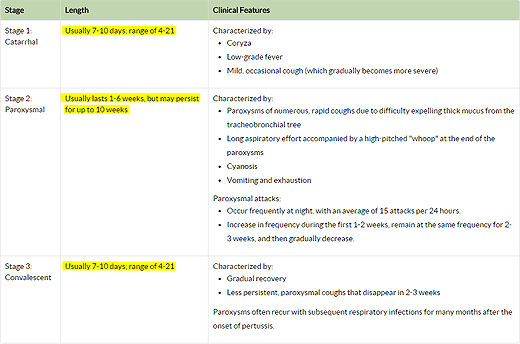
Homeopaths believe that repeatedly diluting a substance in water makes it stronger because water retains “memory” of the substance. Chiropractors believe disease results from disruption of the flow of a life force from the brain through the spinal nerves caused by misalignments of the vertebrae. These beliefs are both scientifically false, and absurd on their face. But they aren’t the wackiest thing I’ve ever heard. That distinction goes to this gem written by Heather Dexter, the mother who let her children suffer 6 months of horror from pertussis, coughing and gasping for breath, in order to stroke her own ego as a naturopath.
[pullquote align=”right” color=”#c6490e”]”Turns out the best way to clear out the lungs is through the rectum … enemas.”[/pullquote]
Heather informed us:
Turns out the best way to clear out the lungs is through the rectum … enemas.
That got me thinking about the centrality of enemas in alternative health. It turns out that I’m not the only one who has pondered this. Dr. Edzard Ernst, who has spent his career debunking pseudoscience, has written on this topic in Colonic Irrigation and the Theory of Autointoxication: A Triumph of Ignorance over Science
Colonic irrigation is an enema on steroids. Whereas an enema involves a one time administration of fluid by rectum to clean the last third of the colon, colonic irrigation involves literally irrigating (or attempting to irrigate) the entire colon. In both cases, the theory is based on the belief in auto-intoxication:
The theory of autointoxication claims that by-products of incomplete digestion may poison the body and, therefore, cause disease. It can be traced back to most ancient cultures of medicine. In the Western world, humoral medicine was based on the idea that all diseases were caused by the imbalance of the four body humors. Conversely, health constituted a balanced mix of these humors. Waste products formed in the intestinal tract were thought to be a major potential contributor to such imbalance. Both Hippocrates and later Galen viewed “autointoxication” as a major etiologic factor of disease.
The cure for disease followed directly from this belief: physically removing the waste products from the colon would treat any and all diseases.
The theory found particular favor in the 19th Century:
Charles A. Tyrell was particularly aggressive in promoting … his therapeutic device, the “Cascade”. This was a rubberized water bottle that held 5 quarts of liquid. The patient would insert its nozzle into his or her rectum and sit on the instrument. The patient’s body weight would then create the pressure to drive the fluid into the patient’s colon. Tyrell led huge advertising campaigns promoting his “Cascade” as a cure for anything from cholera to rheumatism. Like most quacks, he emphasized that his treatment was natural and hence harmless… Like most quacks, he promoted his treatment as a veritable panacea without ever providing convincing evidence.
Sound familiar?
It should because the contemporary revival of the enema owes much to the same beliefs and marketing practices:
Today colon therapy is almost as popular as it was in its heyday. It forms an integral part of the therapeutic armamentarium of most (nonmedically qualified) alternative practitioners around the world who have, during the past three decades, experienced an unprecedented resurgence in this popularity…
Many of the outlandish claims of yesterday are echoed today … [T]he therapy cleans the colon in its full length, detoxifies it, reconstitutes intestinal flora, and even rids the body of parasites and prevents bacteria from entering the blood stream. Today’s list of indications for colon therapy is impressive: alcoholism, allergies, arthritis, asthma, backache, bad breath, bloating, coated tongue, colitis, constipation, damage caused by nicotine or other environmental factors, fatigue, gas, headache, hypercholesterolemia, hypertension, indigestion, insomnia, joint problems, liver insufficiency, loss of concentration, mental disorders, parasite infestation, proneness to infections, rheumatoid arthritis, sinus congestion, skin problems, and ulcerative colitis.
And apparently pertussis, too.
It’s rather remarkable considering the fact that in the intervening years we discovered the germ theory of disease, antibiotics and surgical treatment for or excision of diseased organs. But alternative health is still living in the age of evil humors and treatments that require no special knowledge to recommend or perform.
Ernst concludes:
False claims, a lack of evidence, big money, aggressive advertising, disregard of risk – little seems to have changed.
The importance of enemas in contemporary alternative health shows that he’s absolutely right.