The central conceit of contemporary natural mothering is that mothering in nature (including childbirth and breastfeeding) was perfectly designed and therefore we should emulate it. The “proof” is that we are still here.
But there’s a big difference between the survival of the species and survival of individuals within the species. The reality is that nature views babies as expendable and only women who are insulated from nature by their privilege could wish to copy that.
[perfectpullquote align=”right” bordertop=”false” cite=”” link=”” color=”” class=”” size=””]In Nature 27% of babies died in their first year and 47.5% did not survive to puberty.[/perfectpullquote]
One of the main characteristics of reproduction in the animal kingdom (and the plant kingdom) is massive wastage. The chance of any individual organism surviving to adulthood is very small; therefore, massive amounts of offspring must be produced because most of them are naturally going to die.
Think about how many seeds are produced by an individual plant. Think about how many larvae are produced by one insect. Think about how many eggs are produced by an individual fish. Then think about how many of those survive to become the adult form: only a vanishingly small proportion. There’s a big difference between survival of the species and survival of individuals within the species.
The classic example is the thousands of baby turtles who all hatch on a single night and immediately begin clambering across the beach to safety in the sea. Along the way they must travel a gauntlet of predators and most will not survive. There’s a big difference between survival of the species and survival of individuals within the species.
How about those animals that invest time in brooding or gestating their young? For them, parental energy expenditure is much greater and the the proportion of offspring that are lost before adulthood is consequently much lower, but it is still high.
How high?
According to the paper Infant and child death in the human environment of evolutionary adaptation:
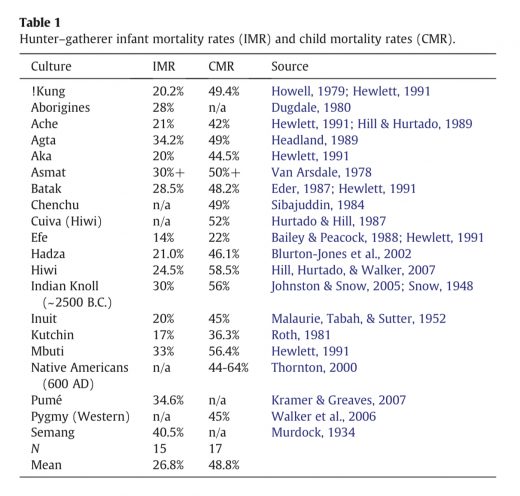
We examine a large number of both hunter–gatherer (N=20) and historical (N=43) infant and child mortality rates to generate a reliable quantitative estimate of their levels … Using data drawn from a wide range of geographic locations, cultures, and times, we estimate that approximately 27% of infants failed to survive their first year of life, while approximately 47.5% of children failed to survive to puberty … a cross-species comparison found that human child mortality rates are roughly equivalent to Old World monkeys, higher than orangutan or bonobo rates and potentially higher than those of chimpanzees and gorillas.
This chart demonstrates the horrific infant and child mortality rates in indigenous cultures:
There’s a big difference between survival of humans as a species and survival of individual humans within the species.
How does this compare with our closest animal relatives?
[A] cross-species comparison found that human child mortality rates are roughly equivalent to Old World monkeys, higher than orangutan or bonobo rates and potentially higher than those of chimpanzees and gorillas.
In other words, astronomical rates of infant and child mortality are not merely natural, they’re quite common among primates.
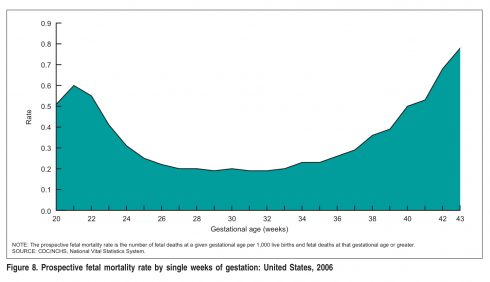
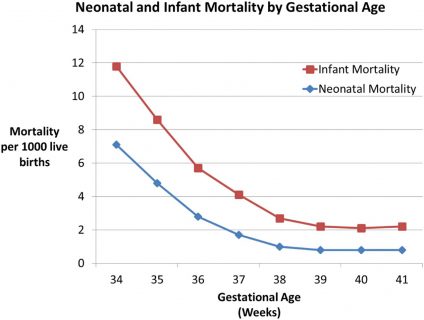
Childbirth and breastfeeding aren’t “perfectly designed.” They’re relatively poorly designed. In contrast, the interventions of modern obstetrics ARE designed to save close to 100% of babies. That’s why modern infant mortality is only a small fraction of natural infant mortality.
Similarly, infant formula IS designed to save as close to 100% of babies as possible and vaccinations ARE designed to save as close to 100% of children as possible.
That’s why contemporary US child mortality is only a tiny fraction more than infant mortality.
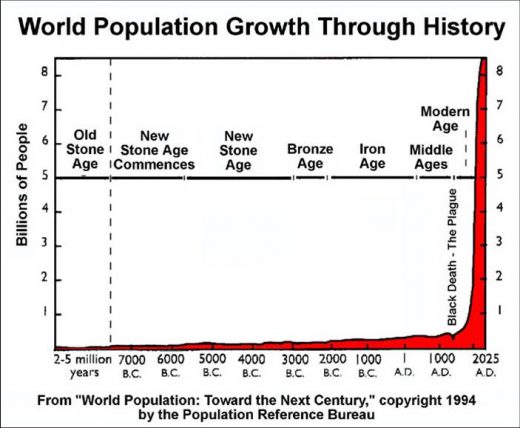
This graph represents the dramatic increase in population that has resulted from technology:
Natural mothering advocates want to return to Nature in the Paleolithic (Stone Age) because —supposedly — childbirth and breastfeeding are “perfectly designed” and “we are still here.”
Nature views babies as expendable, subject to the exact same natural forces that kill babies of other species. The difference between humans and all other animals — the reason we have thrived and expanded to take over the planet — is NOT that humans are perfectly designed for nearly 100% survival in birth or that breastfeeding is perfectly designed to support 100% of infants. The difference is that we use technology to ensure that babies who would otherwise die will live instead.
Natural childbirth advocates who prattle that women are perfectly designed to give birth and lactivists who prate that women are perfectly designed to breastfeed successfully live in a fantasy world where “trusting” birth and breastfeeding seems to them to be an actual strategy when it is nothing more than immature, wishful thinking. The irony is that their fantasy world is made possible by the liberal use of the technologies that they deplore.
In Nature 27% of babies died in their first year and 47.5% did not survive to puberty. Those numbers are consistent with other primates. Nature views babies (and children) as expendable. Only a privileged fool would want to emulate that.