Maria Kang is shocked, shocked that anyone could have misinterpreted her “playful” suggestion as hate speech.
Kang has sparked internet discussion with this image, posted on her Facebook page:

And like other vicious women taken to task for making women feel bad, she thinks SHE is the one who is being discriminated against:
Will a “real woman” please stand up? In the age of Photoshop, plastic surgery and celebrity idolatry, it seems women are constantly debating what is considered a “real” woman. And, as I found out recently when I posted a picture of myself looking fit and healthy in workout clothes with my three sons (playfully asking the question “What’s your excuse?”), apparently I don’t count. My voice as an apparently nonreal woman counts so little, in fact, that Facebook recently banned me temporarily from the site — shutting down my account for almost three days for supposedly violating the site’s terms of service — after a number of users flagged a post of mine venting about the damaging culture of fat acceptance. After my post had garnered thousands of likes, comments and shares, these users apparently reported what I wrote as “hate speech.”
Maria is right. Her image is not hate speech. It is hateFUL speech. And it is depressingly familiar. Yet another Western, white, relatively well off woman promotes the notion that women should be judged by the functions of her body, not the power of her mind or the accomplishments she has achieved or the people she has aided.
And like natural childbirth advocates who think women’s virtue is located in her vagina, or lactivists who believe that women’s virtue is embodied in lactating breasts, Maria thinks women’s virtue is determined by how closely they approximate the Western, white ideal of the thin and toned body.
Not suprisingly, King justifies her viciousness by appeals to “science.”
Overweight women are now standing up (often half-naked) in defiance, exclaiming: “I have a beautiful ‘curvy’ body” and “This is what a real woman looks like.” These campaigns send a message that being overweight is normal…
Constant campaigns promoting self-acceptance and embracing one’s curves are placing the psychological need for a positive body image ahead of health. When you normalize a problem you create complacency. After all, you can’t fix a problem if you don’t see a problem…
Sound familiar? It should. Consider the lactiviciousness of Allison Dixley, the self-proclaimed “Alpha Parent”. She posted this gem:
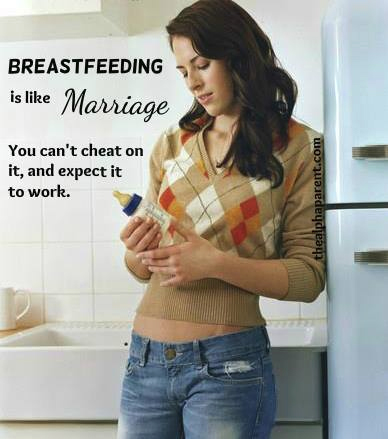
Wow, what a coincidence! This picture also depicts a Western, white woman who is thin and toned.
And she also attempts to justify a hateful meme.
Aside from the important supply-related issues, there is also the fact that combination feeding dilutes much of the protection afforded by breastfeeding the way nature intended … To use the marriage analogy: a marriage can still exist when cheating has occurred; likewise breastfeeding can still exist when supplementation has occurred, but it will not ‘work’ as nature intended. Both mother and baby will not reap the normal physiological advantages.
Yet another startling coincidence! Both women justify their viciousness by appeals to “the science”; King appeals to “the science” about obesity and Dixley to “the science” about breastfeeding.
Charlotte Faircloth, a sociologist of parenting, has written about the abuse of science by lactivists (‘What Science Says is Best’: Parenting Practices, Scientific Authority and Maternal Identity) and her words have relevance for Kang’s abuse of “the science” of obesity.
When ‘science’ says something is healthiest for infants, it has the effect, for [lactivists], of shutting down debate; that is, it dictates what parents should do…
… [U]nder the assumption that science contains ‘no emotional content’, a wealth of agencies with an interest in parenting – from policy makers and ‘experts’ to groups of parents themselves – now have a language by which to make what might better be termed moral judgements about appropriate childcare practices. [But] ‘Science’ is not a straightforward rationale in the regulation of behaviour, rather, it is one that requires rigorous sociological questioning and debate in delimiting the parameters of this ‘is’ and the ‘ought’.
Kang, who judges women by their weight, justifies it with a similar appeal: it’s okay to be vicious to overweight women because being thin is “healthier.” Leave aside for the moment the fact that the scientific evidence actually shows that being slightly overweight is healthiest. The point is that both Dixley and Kang are exponents of health moralism, the practice of moralizing personal choices by appeals to “health.”
This is just an new gloss on an old phenomenon, the locating of women’s value and worth in the function or appearance of their bodies.
It is long past time for us to take a stand against viciousness masquerading as concern about health. Do we want our daughters to believe that their worth resides exclusively between in their breasts, across their flat, toned abdomens and in their vagina? Or do we want our daughters (and our sons!) to recognize that their worth is in the content of their character, the way they use their natural gifts, and how they treat others, including others who differ from themselves?
Here’s the meme I’d like to see:

I’m not holding my breath, though. Images that question privilege are not nearly as popular as those that further entrench it.
*Someone pointed out to me that Kang is Asian-American. Nonetheless, she promotes the Western, white, well off ideal of the female body.