Homebirth had a perfect record in 2013.
Not a single scientific paper or set of state, national or international statistics showed homebirth to be safe!
And, of course, the Midwives Alliance of North America (MANA), the organization that represents homebirth midwives, continued to hide its own death rates.
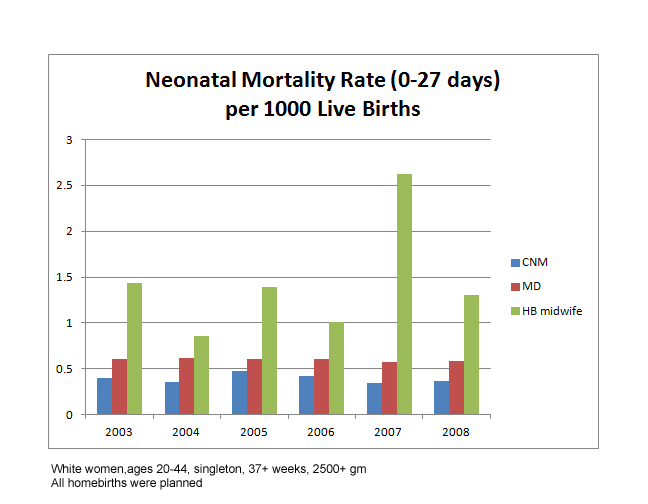
1. New CDC statistics, same old increased homebirth death rate. The dramatic increase in homebirth death rates has been remarkably consistent over the years.
Keep in mind that these statistics dramatically undercount the real rate of homebirth death. Why?
a. All homebirth transfers are included in the MD numbers. That means that any deaths that occurred after the mother was transferred to the hospital are in the MD group and not in the homebirth group where they belong. This is important because we know that many homebirth deaths occur because even being “10 minutes from the hospital” is not close enough to save a baby in a life threatening emergency.
b. Intrapartum deaths are not included in these statistics at all, because those babies don’t get birth certificates. All those homebirths where dead babies drop into the hands of unsuspecting homebirth midwives (“the heart rate was just fine a minute ago”) are not noted here.
2. Oregon releases official homebirth death rates, and they are hideous.
You may recall that back in August 2010, Melissa Cheyney, the Director of Research for the Midwives Alliance of North America (MANA) and also the head of the Board of Direct Entry Midwifery, rejected a call by the State of Oregon for access to the MANA homebirth death rates for Oregon. As a result, the State decided to collect the statistics themselves. They turned to Judith Rooks, a certified nurse midwife and midwifery researcher who is known to be a supporter of direct entry midwifery, to analyze the Oregon homebirth statistics for 2012.

As Rooks regretfully acknowledged:
Many women have been told that OOH births are as safe or safer than births in hospitals…
But out-of-hospital births are not as safe as births in hospitals in Oregon, where many of them are attended by birth attendants who have not completed an educational curriculum designed to provide all the knowledge, skills and judgment needed by midwives who practice in any setting.
The death rate is horrific, even AFTER Rooks inappropriately eliminated the death of a baby at homebirth who had congenital anomalies. Since the hospital group contains congenital anomalies, it is not appropriate to remove them the homebirth group.
3. How have professional homebirth advocates responded to the Oregon data. By and large they have ignored it since they can’t refute it or defend it. Jennifer Margulis (whose husband is a lay member of the Oregon Board of Direct Entry Midwifery) did try, however with the stupidest excuse for homebirth deaths ever:
Oregon has some of the safest best homebirth stats in the country IF YOU DON’T COUNT PORTLAND …
Duh. Homebirth is apparently very safe if you just remove the dead babies from your calculations. And what reason does Margulis provide for removing Portland from the calculations? None, of course. She hoping that homebirth advocates are stupid enough to be persuaded by that inane excuse, or, worse still, perhaps she actually believes that it is a valid excuse.
4. New analysis from Arizona shows — yet again — that homebirth triples the neonatal death rate.
What did they find?
Pooled results indicated that homebirths attended by midwives were associated with increased risks for neonatal deaths [pooled OR (95%CI): 3.11 (2.49, 3.89)]. There were no significant differences in outcome of home or hospital births attended by midwives for the other child health measures.
Homebirth increases the risk of neonatal death by a factor of 3 or more.
For mothers, homebirth poses a much lower risk of interventions and the complications that may arise from those interventions. But that advantage is purchased at the price of increased risk of neonatal death, demonstrating yet again that much of obstetrics is preventive medicine, designed to prevent neonatal deaths … and that’s exactly how it works. Give birth at home and you are twice as likely to avoid interventions, but three times as likely to end up with a dead baby as the result.
5. On the international front, the results are much the same. Dutch midwives struggle to avoid accountability for high perinatal death rate.
According to a leading professor of midwifery:
Maternity care in general in The Netherlands has come under scrutiny by governments, media, the public and care providers themselves after two consecutive European Perinatal Statistical Reports ranked The Netherlands among those with the highest rates of perinatal and neonatal mortality compared to other members of the European Union (and Norway) …
… We have learned that infants born to women of low risk whose labour started in primary care with midwives had higher rates of perinatal death associated with delivery compared to those beginning labour in secondary care …
Ank de Jonge, the leading apologist for Dutch midwifery, attempts to avoid responsibility for the high perinatal mortality rate, but actually finds the opposite. After restricting the analysis to term births, de Jonge found that the Netherlands has one of the worst perinatal mortality rates in Western Europe, although now they have the sixth worst rate, instead of the third worst rate.
In other words, de Jonge confirmed that there is a serious problem with perinatal mortality in the Netherlands including the perinatal mortality rate at term. She confirmed that there is significant evidence that Dutch midwives bear responsibility for the Netherlands poor perinatal mortality rate.
De Jonge tried again in another paper that utterly misrepresents her own findings.
6. De Jonge is at it again, slicing and dicing data in yet another unsuccessful attempt to show that homebirth is safe.
De Jonge compared the number of women who SURVIVED severe complications at homebirth to the number of women who SURVIVED severe complications at hospital birth. She didn’t compare the number of women who EXPERIENCED severe complications in each place. And she didn’t compare how many women DIED at each place. Without that information, de Jonge is not entitled to conclude anything.
Severe maternal morbidity is an appropriate measure of safely ONLY when death rate is zero or nearly zero. If the death rate is not zero, that MUST be taken into account in assessing safety. My Letter to the Editor of the BMJ regarding this inexplicable oversight was published the same day. de Jonge and colleagues have responded, and what do you know, the maternal mortality was NOT zero.
Fewer women in the homebirth group experienced severe acute maternal morbidity, but that’s nothing to crow about if one of them died and might have been saved in the hospital.
7. Elsewhere, Australian midwives boast about terrible homebirth death rate.
Setting a new standard for cluelessness, Australian midwives are proudly presented the results of a publicly funded homebirth program, a program that has a homebirth death rate 5X higher that of term hospital birth.
During the 5 years of the study, there were 1807 women who intended, at the start of labor, to give birth at home. 83% had a homebirth, 52% in water (I have no idea why they mention this except to check women’s performances against the midwifery ideal.) The transfer rate was 17%. The C-section rate was 5.4% and the neonatal death rate was 2.2/1000. That’s more than 5X the rate of 0.4/1000 found in a 2009 report on birth in South Australia.In addition, 2 babies suffered hypoxic ischemic encephalopathy (brain damage due to lack of oxygen).
And that probably undercounts the deaths and complications because reporting was voluntary and only 9 of 13 program directors responded.
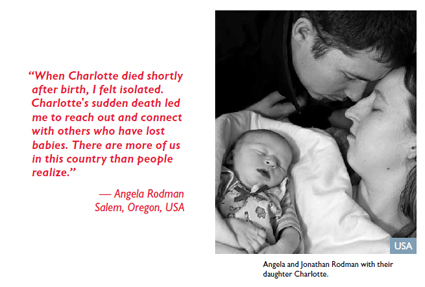
8. Ironically, Save the Children illustrated US neonatal death by using a CPM attended homebirth. The organization (?unwittingly) used a photo that I recognized as a CPM attended homebirth death that was almost certainly preventable.
In other words, the face of first day death in the US is preventable death at homebirth.
9. The most important paper on homebirth published in 2013 showed that homebirth increases the risk of a 5 minute Apgar score of zero by nearly 1000%!
Grunebaum et al. found:
Home births (RR 10.55) and births in free-standing birth centers (RR 3.56) attended by midwives had a significantly higher risk of a 5-minute Apgar score of zero (p<.0001) than hospital births attended by physicians or midwives. Home births (RR 3.80) and births in free-standing birth centers attended by midwives (RR 1.88) had a significantly higher risk of neonatal seizures or serious neurologic dysfunction (p<.0001) than hospital births attended by physicians or midwives.
The Grunebaum paper is well done and extremely difficult to undermine. There is simply no question that the data shows that homebirth raises the risk of a 5 minute Apgar score of 0 by nearly 1000%. The authors’ decision to use the 5 minute Apgar score of zero is truly inspired. Other research shows that homebirth has an appalling rate of intrapartum death, and not just any intrapartum death, but totally unexpected (“the heart rate was normal right up until the baby was born”) death. This is almost certainly due to failure to monitor babies appropriately during labor. The decision to use the 5 minute Apgar score of 0 means that we are looking at severe intrapartum compromise, almost certainly resulting in death.
Most professional homebirth advocates have ignored it, but not MANA. They’ve published a “critique” that contains at least one bald face lie and many more untruths.
10. And how about the death rates of MANA’s own members? Melissa Cheyney continues to spews BS to justify hiding them.
On October 24, ahead of the MANA13 national conference, Cheyney claimed that the MANA statistics cannot be released without the approval of an IRB (institutional review board). First, MANA itself has published almost all the data from the database EXCEPT the death rates. Second, while IRB approval could be required for publications based on the data, IRB approval is not required to read and review the data.
As recently as September 29, Wendy Gordon claimed that there were no articles in press, but on October 24, Cheyney suddently announced there are two papers on the MANA statistics that will be published in the Jan/Feb 2014 issue of the Journal of Midwifery and Women’s Health.
I’m sure that Cheyney will do something to hide the hideous death rate at CPM attended homebirth. I’m so sure, in fact, that if I’m wrong, I will publicly apologize to Cheyney and donate $100 to the MANA stats project.
It’s a win-win for me. If I’m wrong, and Cheyney publishes the number of homebirth deaths compared to the total number of attempted homebirths, I’ll finally have access to the data. If I’m right, I’ll save $100 and I’ll be able to say that you heard it here first that MANA would try to hide the many homebirth deaths at the hands of their members.
Be sure to read the companion piece 2013: The year in homebirth deaths and disasters.